Discover and read the best of Twitter Threads about #bladdercancer
Most recents (16)

@TumorBoardTues @PGrivasMDPhD 1/17 #TumorBoardTuesday #UrothelialCancer #OncTwitter @PGrivasMDPhD
73yo 👴🏼
PMH: HTN, CKD stage 3 (GFR 40), hearing loss
2 month hx flank pain, urinary hesitancy, & hematuria
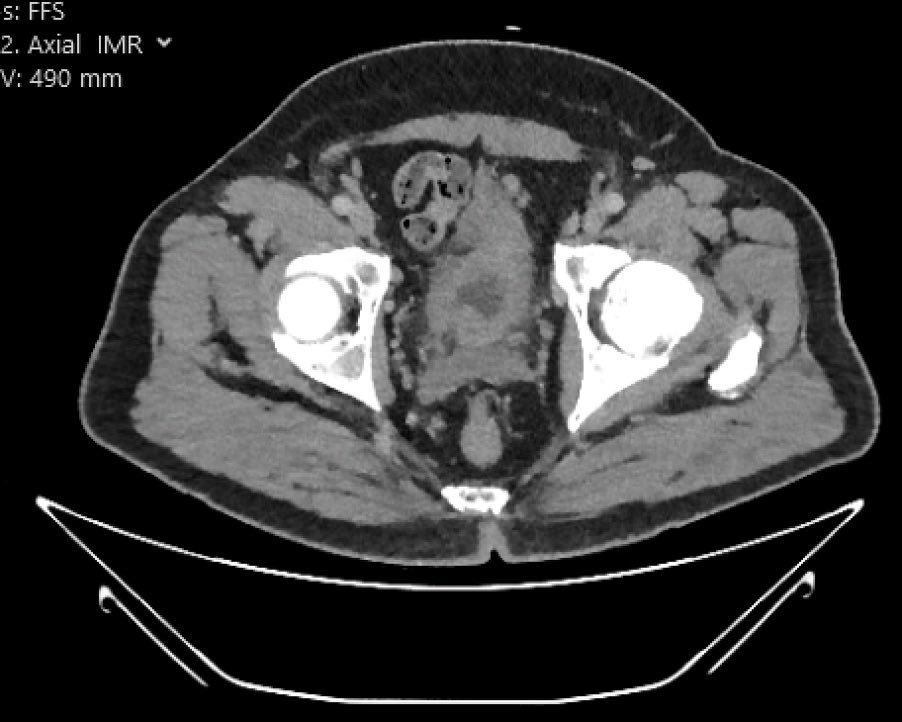
🩻CT chest abd/pelvis: focal mass-like thickening of anterior bladder wall; no LN-pathy or other mets
73yo 👴🏼
PMH: HTN, CKD stage 3 (GFR 40), hearing loss
2 month hx flank pain, urinary hesitancy, & hematuria
🩻CT chest abd/pelvis: focal mass-like thickening of anterior bladder wall; no LN-pathy or other mets
@TumorBoardTues @PGrivasMDPhD 2/17 #TumorBoardTuesday #UrothelialCancer #BladderCancer @MPishvaian @JohnEbbenMDPhD @OncoAlert @BCMCancerCenter
👴🏼 underwent TURBT
🔬biopsy: high grade urothelial carcinoma, micropapillary variant (100%) with involvement of muscularis propria
🧐 What would you do for this pt?
👴🏼 underwent TURBT
🔬biopsy: high grade urothelial carcinoma, micropapillary variant (100%) with involvement of muscularis propria
🧐 What would you do for this pt?
@TumorBoardTues @PGrivasMDPhD @MPishvaian @JohnEbbenMDPhD @OncoAlert @BCMCancerCenter @Daniel_J_George @BlkBoiScientist @SimaPorten @dawood_findakly @mtsiatas @TomJayram @arnabguonc @KidneyCancerDoc @HHammersMD @arihakimi @AmandaNizamMD @montypal @brian_rini @shilpaonc @DrYukselUrun @TiansterZhang @fuatbcr @UROncDoc @KNJobanputra @minaseconomides @DrRosenbergMSK

1/5 #TumorBoardTuesday
🧬No more waiting! Here’s our summary of @RachelRiechelm2 @jessrzanotti’s talk re: hypermut #NET. Can biomarker become clinically actionable?
🆓#CME: 2 quick❓
ALL CME 🔗: integrityce.com/TBT2023
CME eval🔗: integrityce.com/TBTeval231/5 #TumorBoardTuesday twitter.com/i/web/status/1…
🧬No more waiting! Here’s our summary of @RachelRiechelm2 @jessrzanotti’s talk re: hypermut #NET. Can biomarker become clinically actionable?
🆓#CME: 2 quick❓
ALL CME 🔗: integrityce.com/TBT2023
CME eval🔗: integrityce.com/TBTeval231/5 #TumorBoardTuesday twitter.com/i/web/status/1…
2/5 #TumorBoardTuesday
Case🎀
Take🏠 messages:
✅ Hypermut(TMB>10) RARE in NET
✅ Post-tx w alkylator (CAPE/TEM)
✅Mixed results w IO monotx; studying dual IO, combos
✅ Repeat NGS if NET becomes more aggressive; ID new targets, hypermut
📚The thread: threadreaderapp.com/thread/1653549…
Case🎀
Take🏠 messages:
✅ Hypermut(TMB>10) RARE in NET
✅ Post-tx w alkylator (CAPE/TEM)
✅Mixed results w IO monotx; studying dual IO, combos
✅ Repeat NGS if NET becomes more aggressive; ID new targets, hypermut
📚The thread: threadreaderapp.com/thread/1653549…
3/5 #TumorBoardTuesday
Case🎀
🎥 TBT in a video
@RachelRiechelm2 shared key points:
✅NGS critical in NETs–change substantially over time!
✅Hypermut after CAPE/TEM more common than we think
✅Strategies that use dual IO are under active investigation- may be more effective!
Case🎀
🎥 TBT in a video
@RachelRiechelm2 shared key points:
✅NGS critical in NETs–change substantially over time!
✅Hypermut after CAPE/TEM more common than we think
✅Strategies that use dual IO are under active investigation- may be more effective!

@TumorBoardTues 1/15 #TumorBoardTuesday #BladderCancer #OncTwitter
75yo👴🏽
HTN: Amlodipine
T2DM: Metformin, Insulin
6 mo: haematuria & weight loss
CTCAP: thickened bladder wall with L side hydronephrosis & borderline paraaortic LNS. No distant mets
TURBT: G3 PT2N1M0 bladder TCC
CrCl: 75ml/min
75yo👴🏽
HTN: Amlodipine
T2DM: Metformin, Insulin
6 mo: haematuria & weight loss
CTCAP: thickened bladder wall with L side hydronephrosis & borderline paraaortic LNS. No distant mets
TURBT: G3 PT2N1M0 bladder TCC
CrCl: 75ml/min
@TumorBoardTues 2/15 #TumorBoardTuesday #BladderCancer @tompowles1 @MPishvaian @JohnEbbenMDPhD
👴🏽 Patient opts for cystectomy.
🤔 Should we do a PET scan prior to surgery? Why or why not?
👴🏽 Patient opts for cystectomy.
🤔 Should we do a PET scan prior to surgery? Why or why not?
@TumorBoardTues @tompowles1 @MPishvaian @JohnEbbenMDPhD 3/15 #TumorBoardTuesday #BladderCancer
❌PET scan prior to✂️
🩻PET lacks sensitivity in MIBC (70% in prior study n=43)
📚@adamkibel_uro pubmed.ncbi.nlm.nih.gov/19652070/
clinically negative CT + bone scan, PET/CT had SNS of 70% in MIBC
🧑🏻⚕️🤝👴🏽 #SharedDecision 4 cycles neoadju gem+cis
❌PET scan prior to✂️
🩻PET lacks sensitivity in MIBC (70% in prior study n=43)
📚@adamkibel_uro pubmed.ncbi.nlm.nih.gov/19652070/
clinically negative CT + bone scan, PET/CT had SNS of 70% in MIBC
🧑🏻⚕️🤝👴🏽 #SharedDecision 4 cycles neoadju gem+cis



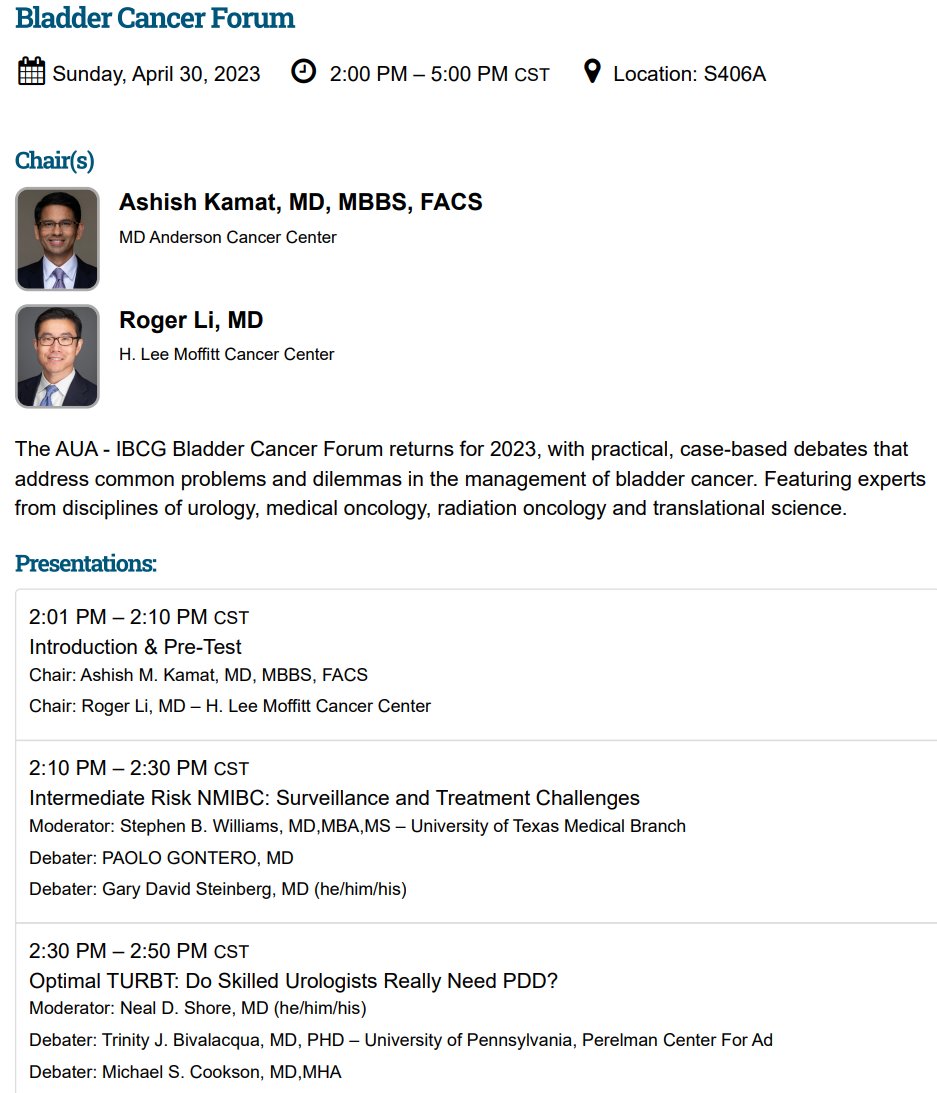
Join us at #AUA23 for our
2nd AUA-IBCG #BladderCancer Forum
Sun, April 30th 2 - 5 pm
@UrogerliMD @paolo_gontero @garysteinbergmd @SWilliams_MD @uromc @tbivala1 @spsutkaMD @SimaPorten @bbmdmsk @AStenzl @JoshMeeks @WesKassouf @PGrivasMDPhD @nnavai @MaxKates @shilpaonc @MariaJRibal
2nd AUA-IBCG #BladderCancer Forum
Sun, April 30th 2 - 5 pm
@UrogerliMD @paolo_gontero @garysteinbergmd @SWilliams_MD @uromc @tbivala1 @spsutkaMD @SimaPorten @bbmdmsk @AStenzl @JoshMeeks @WesKassouf @PGrivasMDPhD @nnavai @MaxKates @shilpaonc @MariaJRibal

Let's get some polls going to help our debaters! #AUA23 #AUA2023 @IBCG_BladderCA @AmerUrological @uromc @tbivala1 @joanfundi @siadaneshmand @JimCatto @UrogerliMD @SWilliams_MD @urotoday @BladderCancerUS
Poll #1a Optimal TURBT:
Do Skilled Urologists Really Need PDD for TURBT?
Poll #1a Optimal TURBT:
Do Skilled Urologists Really Need PDD for TURBT?
Poll #1b Optimal Cystoscopy:
Do Skilled Urologists Really Need PDD for Surveillance Cystoscopy in Clinic?
#AUA23 #AUA2023 @AmerUrological @uromc @tbivala1 @siadaneshmand @MRoupret @UrogerliMD @SWilliams_MD @urotoday @BladderCancerUS @SimaPorten @drtanws @bbmdmsk @MaxKates
Do Skilled Urologists Really Need PDD for Surveillance Cystoscopy in Clinic?
#AUA23 #AUA2023 @AmerUrological @uromc @tbivala1 @siadaneshmand @MRoupret @UrogerliMD @SWilliams_MD @urotoday @BladderCancerUS @SimaPorten @drtanws @bbmdmsk @MaxKates
No monkeying around!
👨🏻⚕️@tompowles1 @drfrankiejs👩🏼⚕️may be in UK, but they’re leading #TumorBoardTuesday on Tuesday!
📅03.28.23 at 8pm ET/12am BT
📰1L pembro or Nivo+Cabo?
🐵While case is finalized, collect FREE #CME (AMA & MOC)
🐒integrityce.com/tbt🙊#OncTwitter #RenalCancer
👨🏻⚕️@tompowles1 @drfrankiejs👩🏼⚕️may be in UK, but they’re leading #TumorBoardTuesday on Tuesday!
📅03.28.23 at 8pm ET/12am BT
📰1L pembro or Nivo+Cabo?
🐵While case is finalized, collect FREE #CME (AMA & MOC)
🐒integrityce.com/tbt🙊#OncTwitter #RenalCancer

@tompowles1 @drfrankiejs @MPishvaian @minaseconomides @JohnEbbenMDPhD @JineshGheeya @niklas_kluemper @EHeath4100 @Heer_Lab @MariaChiaraMCS @ReisLO @PGrivasMDPhD A tad bit of 🙊monkeying around in #TumorBoardTuesday land by attaching a sneak peak into @JohnEbbenMDPhD's wrap up image. 😉
The info is the same!
📅Tues 03/28/23
🕰️8pm ET/12am BT
☕️Cuppa with🇬🇧@tompowles1 👨🏻⚕️👩🏼⚕️@drfrankiejs
🗞️1L tx decision for #RenalCancer
#Urology @Uromigos
The info is the same!
📅Tues 03/28/23
🕰️8pm ET/12am BT
☕️Cuppa with🇬🇧@tompowles1 👨🏻⚕️👩🏼⚕️@drfrankiejs
🗞️1L tx decision for #RenalCancer
#Urology @Uromigos

Join us here on #TumorBoardTuesday for a UK-led #BladderCancer case from👨🏻⚕️ @tompowles1👩🏼⚕️ @drfrankiejs
📅Tues, 03/28/23 at🕗8PM ET / 12AM 🇬🇧
FREE #CME👉🏽integrityce.com/tbt 👈🏼
💬A way to gather input is with📊, so b4️⃣ their case, tell us where you are in your 🩺 journey
👇🏽
📅Tues, 03/28/23 at🕗8PM ET / 12AM 🇬🇧
FREE #CME👉🏽integrityce.com/tbt 👈🏼
💬A way to gather input is with📊, so b4️⃣ their case, tell us where you are in your 🩺 journey
👇🏽

@TumorBoardTues @TomJayram @arnabguonc @UroCancerMD @vinay_onc @simon_p_kim @AlexAlvaro_PSC @AlyaShamsan @MichaelStaehler @DrOmarMian @kaydaustin @josiegarcia1 @LeeJonesMBA @mcricardoa @UroDocAsh @Uromigos @AJangMD @BenMironMD @ChrisSweens1 @Tanjin097 @NikiTripathi27 1/15 #TumorBoardTuesday #BladderCancer #OncTwitter
71 y/o 👨🏽🦳
Former 🚬
👨🏭Worked in various factories in 80s-00s
Recently diagnosed metastatic #UrothelialCancer (lymph nodes/lung)
🤨 What would you pick for your first line of therapy?
71 y/o 👨🏽🦳
Former 🚬
👨🏭Worked in various factories in 80s-00s
Recently diagnosed metastatic #UrothelialCancer (lymph nodes/lung)
🤨 What would you pick for your first line of therapy?
@TumorBoardTues @TomJayram @arnabguonc @UroCancerMD @vinay_onc @simon_p_kim @AlexAlvaro_PSC @AlyaShamsan @MichaelStaehler @DrOmarMian @kaydaustin @josiegarcia1 @LeeJonesMBA @mcricardoa @UroDocAsh @Uromigos @AJangMD @BenMironMD @ChrisSweens1 @Tanjin097 @NikiTripathi27 2/15 #TumorBoardTuesday
1L treatment for UC
📍cis eligible: SOC is gem/cis
📚pubmed.ncbi.nlm.nih.gov/11001674/
📍Frontline EV+P promising early phase results in cis-ineligible
📚ascopubs.org/doi/abs/10.120…
📍Ongoing ph3 trial: EV+pembro vs gem/cis (or carbo) clinicaltrials.gov/ct2/show/NCT04…
1L treatment for UC
📍cis eligible: SOC is gem/cis
📚pubmed.ncbi.nlm.nih.gov/11001674/
📍Frontline EV+P promising early phase results in cis-ineligible
📚ascopubs.org/doi/abs/10.120…
📍Ongoing ph3 trial: EV+pembro vs gem/cis (or carbo) clinicaltrials.gov/ct2/show/NCT04…



@TumorBoardTues @TomJayram @arnabguonc @UroCancerMD @vinay_onc @simon_p_kim @AlexAlvaro_PSC @AlyaShamsan @MichaelStaehler @DrOmarMian @kaydaustin @josiegarcia1 @LeeJonesMBA @mcricardoa @UroDocAsh @Uromigos @AJangMD @BenMironMD @ChrisSweens1 @Tanjin097 @NikiTripathi27 @PGrivasMDPhD @PauloBergerot @spsutkaMD @shilpaonc @montypal @tompowles1 @NazliDizman 3/15 #TumorBoardTuesday
Checkpoint☑️
✅Pembrolizumab: approved as single agent for those NOT eligible for platinum chemotherapy
📚thelancet.com/journals/lanon…
BUT
✨KEYNOTE-361: adding pembro to platinum based chemo did NOT result in PFS/OS improvement
📚thelancet.com/journals/lanon…
Checkpoint☑️
✅Pembrolizumab: approved as single agent for those NOT eligible for platinum chemotherapy
📚thelancet.com/journals/lanon…
BUT
✨KEYNOTE-361: adding pembro to platinum based chemo did NOT result in PFS/OS improvement
📚thelancet.com/journals/lanon…



@TumorBoardTues @drteplinsky @stolaney1 @hoperugo @dradityabardia @BreastCaupdates @BCRFcure @MBCNbuzz 2/5 #TumorBoardTuesday
Take🏠msgs:
✅HER2 low= 1+ to 2+ IHC, -FISH
✅T-Dxd approved in 1L HER2 low
✅Watch tox, esp ILD (need reg CT thorax)!
✅TROP-2 ADCs an option (Sacituzumab govitecan); choose based on pt profile, agent tox
📚@drteplinsky’s thread:
threadreaderapp.com/thread/1623124…
Take🏠msgs:
✅HER2 low= 1+ to 2+ IHC, -FISH
✅T-Dxd approved in 1L HER2 low
✅Watch tox, esp ILD (need reg CT thorax)!
✅TROP-2 ADCs an option (Sacituzumab govitecan); choose based on pt profile, agent tox
📚@drteplinsky’s thread:
threadreaderapp.com/thread/1623124…
@TumorBoardTues @drteplinsky @stolaney1 @hoperugo @dradityabardia @BreastCaupdates @BCRFcure @MBCNbuzz 3/5 #TumorBoardTuesday
🎥 TBT in a video
New 1L T-DXd option for patients w #mBC (HER2 low, ER/PR-).
T-DXd is an antibody drug conjugate (ADC), tethering deruxtecan payload to HER2 ab. Improvements over chemo in mOS and PFS, but watch carefully for ILD and all toxicities!
🎥 TBT in a video
New 1L T-DXd option for patients w #mBC (HER2 low, ER/PR-).
T-DXd is an antibody drug conjugate (ADC), tethering deruxtecan payload to HER2 ab. Improvements over chemo in mOS and PFS, but watch carefully for ILD and all toxicities!
@TumorBoardTues @drteplinsky @stolaney1 @hoperugo @dradityabardia @BreastCaupdates @BCRFcure @MBCNbuzz 4/5 #TumorBoardTuesday
📷 TBT in an image
Check out quick proposed tx algorithm for HR+ & HR- HER2 low disease. Since HER2 low is defined as 1+ through 2+ on IHC with - FISH, up to ‼️60%‼️ of cases previously called HER2 NEGATIVE are actually HER2 LOW!
📷 TBT in an image
Check out quick proposed tx algorithm for HR+ & HR- HER2 low disease. Since HER2 low is defined as 1+ through 2+ on IHC with - FISH, up to ‼️60%‼️ of cases previously called HER2 NEGATIVE are actually HER2 LOW!

Join us at #EAU23 for our Rapid Fire Debate #BladderCancer Session
Sat, March 11, 3:15 pm
@MarekBabjuk @joanfundi @paolo_gontero @slernerbcmedu1 @UrogerliMD @MRoupret @LAUrology_NL @ParamMariappan @JBjerggaard @JimCatto @amassonlecomte @DrShariat @AndreaNecchi @AStenzl @Uroweb
Sat, March 11, 3:15 pm
@MarekBabjuk @joanfundi @paolo_gontero @slernerbcmedu1 @UrogerliMD @MRoupret @LAUrology_NL @ParamMariappan @JBjerggaard @JimCatto @amassonlecomte @DrShariat @AndreaNecchi @AStenzl @Uroweb


Help our debaters prep with your responses
Poll #1a: Does PDD/NBI etc help alter natural history of NMIBC?
@joanfundi @MarekBabjuk
Poll #1a: Does PDD/NBI etc help alter natural history of NMIBC?
@joanfundi @MarekBabjuk
@TumorBoardTues @PGrivasMDPhD @MPishvaian @JohnEbbenMDPhD 1/19 #TumorBoardTuesday #BladderCancer #OncTwitter
74 yo🧓🏼
HTN
DM2
2020: localized Rt upper tract urothelial carcinoma
2020: ✂️ radical nephroureterectomy
🧪Germline testing negative
Complicated by CKD stage 4 after ✂️ (creatinine clearance 25 ml/min)
🩻Restaging CT CAP 1 year
74 yo🧓🏼
HTN
DM2
2020: localized Rt upper tract urothelial carcinoma
2020: ✂️ radical nephroureterectomy
🧪Germline testing negative
Complicated by CKD stage 4 after ✂️ (creatinine clearance 25 ml/min)
🩻Restaging CT CAP 1 year
@TumorBoardTues @PGrivasMDPhD @MPishvaian @JohnEbbenMDPhD 🩻 NEW metastatic disease to spine, 🫁 and retroperitoneal lymph nodes
ECOG PS 2
🔬Biopsy of RP lymph node: Metastatic #UrothelialCarcinoma
🧪Molecular: FGFR3-TACC3 fusion, MTAP loss, CDKN2A loss
🤨 What 1L treatment would you pick for this patient?
ECOG PS 2
🔬Biopsy of RP lymph node: Metastatic #UrothelialCarcinoma
🧪Molecular: FGFR3-TACC3 fusion, MTAP loss, CDKN2A loss
🤨 What 1L treatment would you pick for this patient?
@TumorBoardTues @PGrivasMDPhD @MPishvaian @JohnEbbenMDPhD 3/19 #TumorBoardTuesday @PGrivasMDPhD @MPishvaian @JohnEbbenMDPhD #UrothelialCancer
🤔 Is the above 74yo 🧓🏼 patient a good candidate for platinum-based chemotherapy?
🤨 Poll: Which of these criteria would make this patient platinum-ineligible?
🤔 Is the above 74yo 🧓🏼 patient a good candidate for platinum-based chemotherapy?
🤨 Poll: Which of these criteria would make this patient platinum-ineligible?

There is an unmet need for effective treatments for #BladderCancer, especially for advanced stages of the disease.
Innovative treatments for bladder cancer have the potential to capture a significant share of the market.
Innovative treatments for bladder cancer have the potential to capture a significant share of the market.
Bladder #cancer is a common and costly disease, with over 600,000 new cases diagnosed worldwide each year. This high prevalence of the disease creates a large potential market for treatments.
Saw this article on #Theralase in @YahooFinance:
finance.yahoo.com/news/theralase…
Saw this article on #Theralase in @YahooFinance:
finance.yahoo.com/news/theralase…
Theralase is a biotech company focused on the research, development, and commercialization of advanced medical technologies, with the potential to be used in a wide range of medical applications, including the treatment of cancer, arthritis, and other diseases
What do you think?
What do you think?

Pre-print alert 🚨 New story from my lab "The cytidine deaminase APOBEC3G drives cancer mutagenesis and clonal evolution in bladder cancer" This is one of the first projects in my lab, so I am thrilled to see it come to fruition 🐁🧪 🔬 #bladdercancer #biology @OncoAlert


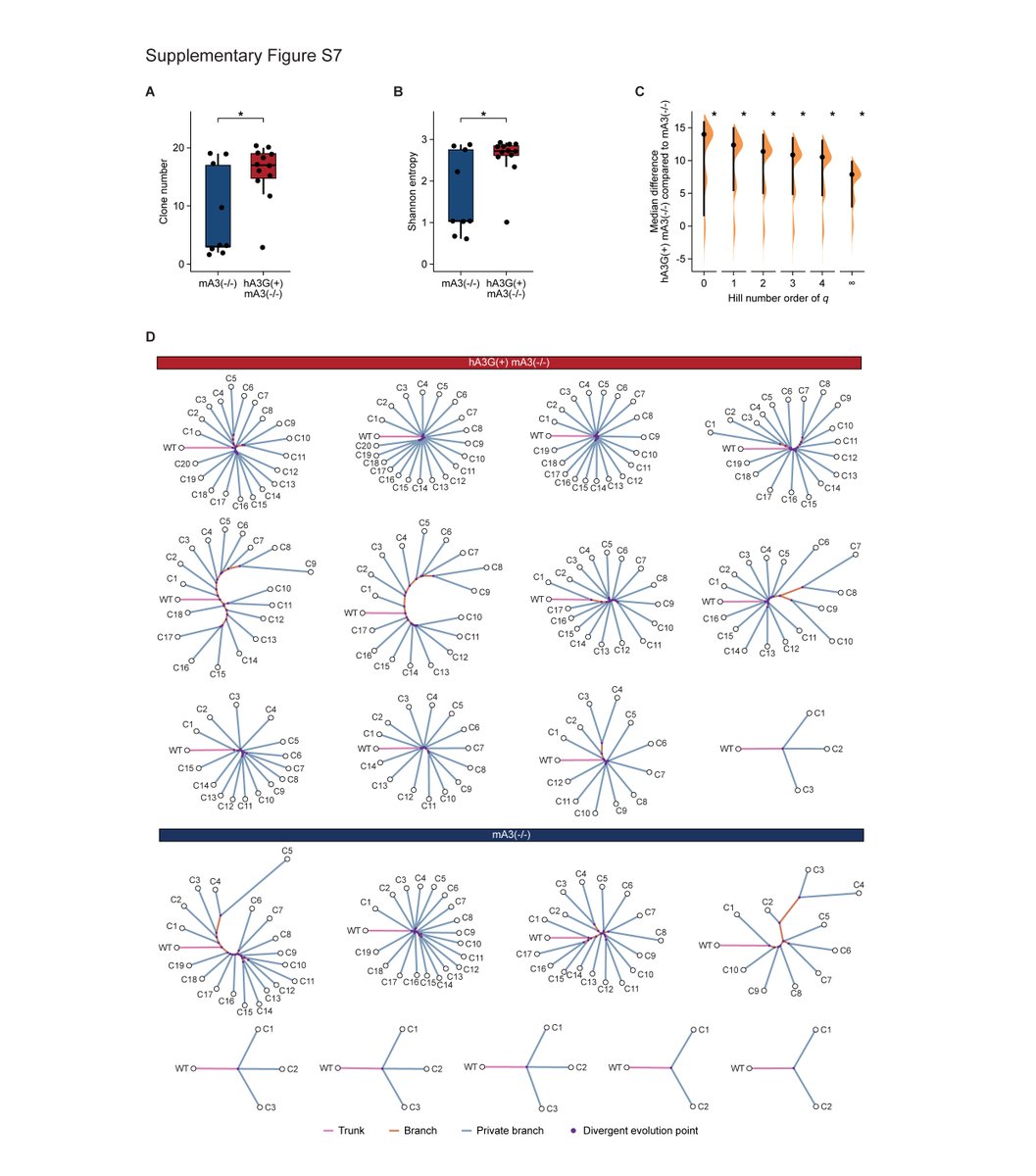
Led by postdoc @weisi_liu w amazing contributions by @knewtrophil @FKhaniPath @DrLaMontBarlow @DuyDNguyen1 L. Gu K. Eng @BhavneetBhinder @MDUppal92 @ChRecapet @asbonerw S. Ross @ElementoLab @ChelicoUSASK
We previously showed that bladder cancer is characterized by extensive and early divergent evolution.
We also showed that the APOBEC3-like mutational signatures were enriched in chemotherapy-resistant urothelial cancers nature.com/articles/ng.36… @NatureGenet
We also showed that the APOBEC3-like mutational signatures were enriched in chemotherapy-resistant urothelial cancers nature.com/articles/ng.36… @NatureGenet

Alert 🎙Pharmacy Grand Rounds Thread Ahead! 🚨
Last week I had one of my final presentations of the year! With a catchy title😉
Urine for an Update! Updates in the management of metastatic urothelial cancer
Hold your bladders, this is an extensive update! 😂
#oncopharm
Last week I had one of my final presentations of the year! With a catchy title😉
Urine for an Update! Updates in the management of metastatic urothelial cancer
Hold your bladders, this is an extensive update! 😂
#oncopharm

Bladder cancer can be divided into two ✌️subtypes:
1) Non-muscle invasive: encompasses in-situ and localized disease➡️5-yr OS >70%
2) Muscle invasive: encompasses regional or metastatic disease➡️5-yr OS dismal especially for metastatic disease 😔
1) Non-muscle invasive: encompasses in-situ and localized disease➡️5-yr OS >70%
2) Muscle invasive: encompasses regional or metastatic disease➡️5-yr OS dismal especially for metastatic disease 😔

Cisplatin=SOC
50% of pts w are ineligible due to older age👵🏻, poor PS, ⬇️ renal function, ⬇️hearing, neuropathy, heart failure 🫀& other comorbities that ⬆️ risk of ⚠️
Carboplatin yields inferior responses➡️NOT 🙅🏻♀️ an equal alternative due to ⬇️ OS😢➡️pt left w/minimal tx options
50% of pts w are ineligible due to older age👵🏻, poor PS, ⬇️ renal function, ⬇️hearing, neuropathy, heart failure 🫀& other comorbities that ⬆️ risk of ⚠️
Carboplatin yields inferior responses➡️NOT 🙅🏻♀️ an equal alternative due to ⬇️ OS😢➡️pt left w/minimal tx options


Still digesting #bladdercancer trials at #GU21. QUILT 3.032 trial clinicaltrials.gov/ct2/show/NCT03… testing #N803 in BCG-unresponsive CIS was an important result. Safety data appropriate for intravesical therapy – and CR rate was higher than seen with other drugs in similar trials.
1/n
1/n
Note, in case you missed it (as I think most of us did) that the detailed trial results were previously reported as a press release in Dec 2020 yhoo.it/3hfCcWg (unusual for a trial under ASCO embargo?)
2/n
2/n
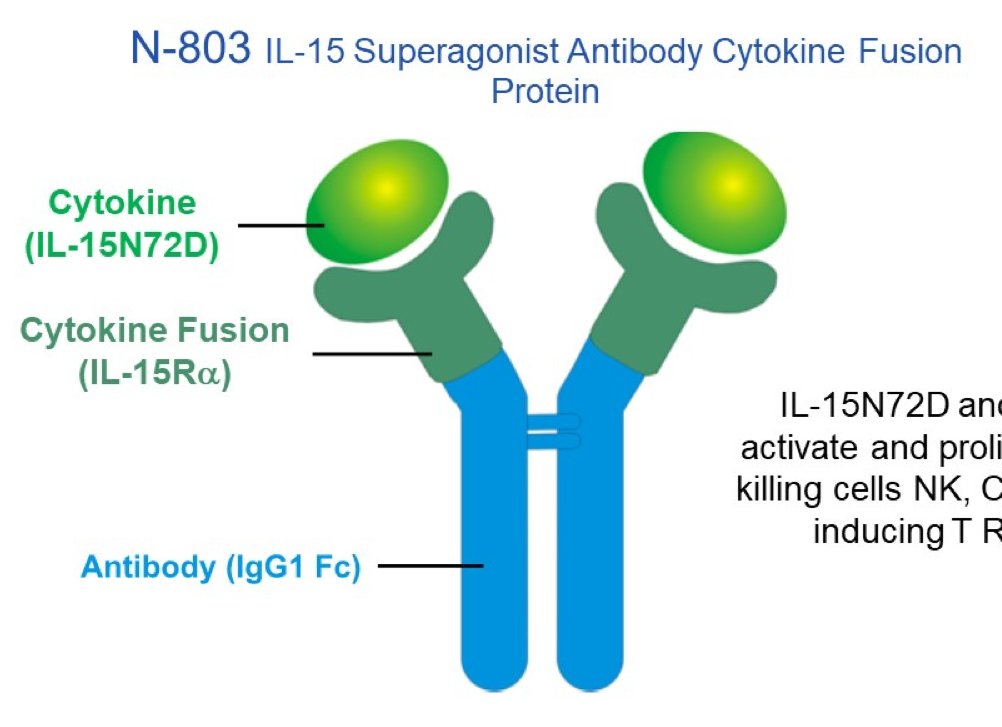
N-803 (aka ALT-803) is a fusion protein: IL15 with N72D mutation (to increase affinity) fused to IL15 receptor (IL15Ra) and IgG1 Fc (improves PK and activity). The resultant IL15 superagonist activates effector NK cells and CD8+ memory T cells, without activation of Tregs.
3/n
3/n

My take on #CheckMate274: Is adj CPI now SOC for #MIUC? Not yet. Here's the design presented today at @ASCO #GU21 - first, thanks to patients & investigators (#DrDeanBajorin, @MattGalsky) who should be commended for completing an adj trial in #bladdercancer - no small feat! (1/9)

First, a trip down memory lane. Here is the data from IMvigor010 - adj atezo v observation. No diff in DFS/OS, period. No difference based on PD-L1 status. Could it be PD-1 v PD-L1? Hard to prove. Could it be obs v pbo control? (2/9)




I stole this slide from @MattGalsky in a separate thread i came across. Here he nicely highlights the attrition on control and experimental arms. IMvigor010 lost a substantial proportion of folks due to "other" reasons on the observation arm. (3/9)


@TheWonkologist: All great & valid points, IMHO we as a #bladdercancer community are just so desperate for an alternative to cystectomy & @FDAOncology already set the bar so low with approval of Pembro in this space that Adstiladrin will almost certainly be FDA approved 1/n
Hopefully, patients declining RC still preferentially go on trials, but with urologists more comfortable managing urinary AEs over IO AEs, Adstiladrin will likely get a higher market share over Pembro (but Gem, GemDoce, MMC might still be used more than both) 2/n
With every drug in this space all showing ~40% 3 m CRs & ~20% 12 m CRs, I worry this is just the natural history of BCG unresponsive #NMIBC. Some slides from a recent talk I gave to @UrologyMSK @SUO_YUO fellows 3/n



Years ago we discovered that FGFR3 alterations are linked with a non-T cell-inflamed immune microenvironment in urothelial #BladderCancer #blcsm (1/6) cancerimmunolres.aacrjournals.org/content/early/…

This finding was replicated in other data sets and suggested that FGFR3-active tumors may be less likely to respond to anti-PD1/L1 #Immunotherapy. It provided a strong rationale for combining FGFR inhibitors with anti-PD-L1 immunotherapy. (2/6)
This hypothesis was refined further by elegant data from @MattGalsky et al, which incorporated TGF-beta and EMT/stromal signatures, which further supported combining FGFR inhibitors and anti-PD-1/L1 (3/6) europeanurology.com/article/S0302-…
