Discover and read the best of Twitter Threads about #MayoIDQ
Most recents (24)

#MayoIDFellowship Core Curriculum Lecture series
Dr. Wengenack asked our fellows to identify this fungi with “spaghetti and meatballs” appearance. #IDBR #MayoIDQ
Dr. Wengenack asked our fellows to identify this fungi with “spaghetti and meatballs” appearance. #IDBR #MayoIDQ

#Malassezia
Microbiologists identify #Malassezia as the “spaghetti and meatball” yeast that causes the prototypical recurrent skin disease, tinea / pityriasis versicolor, characterized by hypo/hyperpigmented plaques and scales, often seen over the back, chest, and neck.
Microbiologists identify #Malassezia as the “spaghetti and meatball” yeast that causes the prototypical recurrent skin disease, tinea / pityriasis versicolor, characterized by hypo/hyperpigmented plaques and scales, often seen over the back, chest, and neck.
#Malassezia species are obligatory lipophilic and requires oil for growth.
BONUS point!
#MicroBoardReview
Name the major zoophilic species of Malassezia that does NOT require lipids for growth.
BONUS point!
#MicroBoardReview
Name the major zoophilic species of Malassezia that does NOT require lipids for growth.
Images of Infectious Diseases
46F with diabetes presents with orbital apex syndrome. Imaging and histopathology shown. What is your differential diagnosis? #MayoIDQ to follow @StephanieGrach @ZYetmar @omarabusaleh15
46F with diabetes presents with orbital apex syndrome. Imaging and histopathology shown. What is your differential diagnosis? #MayoIDQ to follow @StephanieGrach @ZYetmar @omarabusaleh15

2/ #MayoIDQ
46F with uncontrolled DM and recent DKA is admitted because of left sided HA for a month. PE: orbital apex syndrome. Head imaging shown. ENT/neurosurgery proceeded with debridement. Pathology shown. Which one of the following choices is most correct?
46F with uncontrolled DM and recent DKA is admitted because of left sided HA for a month. PE: orbital apex syndrome. Head imaging shown. ENT/neurosurgery proceeded with debridement. Pathology shown. Which one of the following choices is most correct?
3/
Case diagnosis: Rhinocerebral #mucormycosis due to #Rhizopus in a person with poorly controlled diabetes mellitus
Rx:
Surgical debridement
Liposomal #Amphotericin B
Later: transitioned to #Posaconazole upon clinical control and improvement
Case diagnosis: Rhinocerebral #mucormycosis due to #Rhizopus in a person with poorly controlled diabetes mellitus
Rx:
Surgical debridement
Liposomal #Amphotericin B
Later: transitioned to #Posaconazole upon clinical control and improvement
Images of Infectious Diseases
“Food gets stuck in my Adam’s apple”
A 68 year old man presents with weight loss and dysphagia for 6 weeks. Upper endoscopy is shown. What is your diagnosis? #MayoIDQ and case details to follow
“Food gets stuck in my Adam’s apple”
A 68 year old man presents with weight loss and dysphagia for 6 weeks. Upper endoscopy is shown. What is your diagnosis? #MayoIDQ and case details to follow

2/
68M. No PMH. 6w gradual dysphagia to solids with 20 lb weight loss. No F/C/sweats. PE: cachexia. WBC 4.7 Cr 0.9 CXR normal. HBV(-). Rx fluconazole.
Per your suggestion: HIV VL 56K CD4 26. Patient willing to start ART immediately. Genotype pending. You suggest which one?
68M. No PMH. 6w gradual dysphagia to solids with 20 lb weight loss. No F/C/sweats. PE: cachexia. WBC 4.7 Cr 0.9 CXR normal. HBV(-). Rx fluconazole.
Per your suggestion: HIV VL 56K CD4 26. Patient willing to start ART immediately. Genotype pending. You suggest which one?
3/
Case diagnosis: Esophageal candidiasis in a man with newly diagnosed AIDS
Suggested ART: TAF-FTC-bictegravir
ART consists of 2 NRTI in combo with 3rd drug: INSTI, NNRTI or boosted PI.
Among them: INSTI is preferred for various reasons (next)
Case diagnosis: Esophageal candidiasis in a man with newly diagnosed AIDS
Suggested ART: TAF-FTC-bictegravir
ART consists of 2 NRTI in combo with 3rd drug: INSTI, NNRTI or boosted PI.
Among them: INSTI is preferred for various reasons (next)
Images of Infectious Diseases
2 months after visiting family and friends in Manila:
39M. No PMH. One week of fever, chills, cough, pleuritic chest pain, RUQ pain.
Now complains of blurred vision due to endophthalmitis.
Your DDx? #MayoIDQ and case details to follow…
2 months after visiting family and friends in Manila:
39M. No PMH. One week of fever, chills, cough, pleuritic chest pain, RUQ pain.
Now complains of blurred vision due to endophthalmitis.
Your DDx? #MayoIDQ and case details to follow…

2/
39M. No PMH. HIV-. No IDU.
PE: jaundice, endophthalmitis, no dental issues, b/l rales, new systolic murmur, tender RUQ
WBC 18.3 Alk phos 250.
CT chest / abdomen (photo)
TEE: mitral valve vegetation
Which of the following is the most likely pathogen? #MayoIDQ
39M. No PMH. HIV-. No IDU.
PE: jaundice, endophthalmitis, no dental issues, b/l rales, new systolic murmur, tender RUQ
WBC 18.3 Alk phos 250.
CT chest / abdomen (photo)
TEE: mitral valve vegetation
Which of the following is the most likely pathogen? #MayoIDQ
3/
Let us use this case to highlight clinical pearls about liver abscess:
Two major categories
1. Pyogenic liver abscess
2. Amoebic liver abscess
In this case, there are factors that favor pyogenic liver abscess: endocarditis, septic pulmonary emboli and endophthalmitis
Let us use this case to highlight clinical pearls about liver abscess:
Two major categories
1. Pyogenic liver abscess
2. Amoebic liver abscess
In this case, there are factors that favor pyogenic liver abscess: endocarditis, septic pulmonary emboli and endophthalmitis
Images of Infectious Diseases
58M. NYC. No PMH.
1 mo ago: high dose prednisone, rituximab, plasma exchange for presumed paraneoplastic autoimmune polyneuropathy.
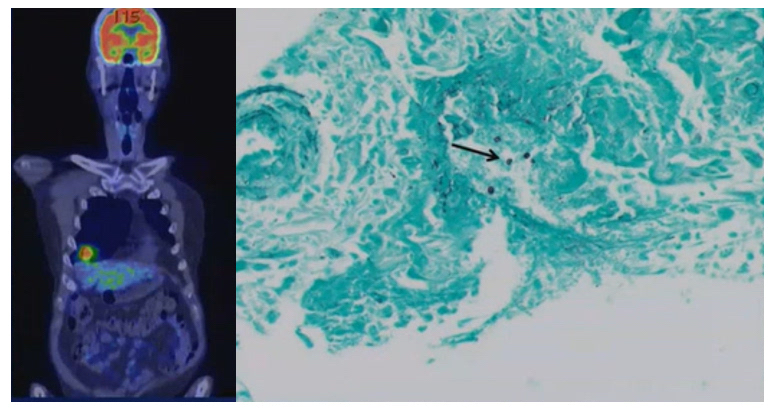
Now: PET-CT. Biopsy (shown)
ROS: fever, cough, chest pain
What is the DDx? Case details #MayoIDQ to follow…
58M. NYC. No PMH.
1 mo ago: high dose prednisone, rituximab, plasma exchange for presumed paraneoplastic autoimmune polyneuropathy.
Now: PET-CT. Biopsy (shown)
ROS: fever, cough, chest pain
What is the DDx? Case details #MayoIDQ to follow…
2/
No travel. No farm exposure. No pets.
Work up:
CXR RML opacity
WBC 13.7. 94%N.
HIV neg.
Galactomannan negative
Histoplasma serology negative
BDG >500
What is the most likely pathogen? #MayoIDQ
No travel. No farm exposure. No pets.
Work up:
CXR RML opacity
WBC 13.7. 94%N.
HIV neg.
Galactomannan negative
Histoplasma serology negative
BDG >500
What is the most likely pathogen? #MayoIDQ
3/
Case diagnosis: #Pneumocystis jirovecii pneumonia presenting as solitary granulomatous inflammatory nodule
BAL PJP smear / PCR negative
Biopsy: PJP
Repeated PCR of stored BALF: low +
Case diagnosis: #Pneumocystis jirovecii pneumonia presenting as solitary granulomatous inflammatory nodule
BAL PJP smear / PCR negative
Biopsy: PJP
Repeated PCR of stored BALF: low +
Images of Infectious Diseases
A young man presents to the ER because of leg numbness. While undergoing evaluation, he had a seizure. CT head is shown (photo). #IDTwitter what is your differential diagnosis?
Case details #MayoIDQ MCQ to follow…
A young man presents to the ER because of leg numbness. While undergoing evaluation, he had a seizure. CT head is shown (photo). #IDTwitter what is your differential diagnosis?
Case details #MayoIDQ MCQ to follow…

2/
36M migrant from Mexico
No PMH. HIV negative.
CC: leg numbness
ED: witnessed seizure
WBC 16. Cr 0.7. AST 35.
CT (photo)
Which one of the following is least likely the correct answer about this condition? #MayoIDQ
36M migrant from Mexico
No PMH. HIV negative.
CC: leg numbness
ED: witnessed seizure
WBC 16. Cr 0.7. AST 35.
CT (photo)
Which one of the following is least likely the correct answer about this condition? #MayoIDQ
3/
Case diagnosis: #Neurocysticercosis NCC due to #Taenia #solium
There was an almost equal spread in the answers (probably due to poorly constructed MCQ :-) )
The least likely correct association is undercooked pork…. which leads to #taeniasis but not directly to NCC
Case diagnosis: #Neurocysticercosis NCC due to #Taenia #solium
There was an almost equal spread in the answers (probably due to poorly constructed MCQ :-) )
The least likely correct association is undercooked pork…. which leads to #taeniasis but not directly to NCC
Images of Infectious Diseases
42M on obinutuzumab for CLL. 4 mo ago: mild COVID-19 - no specific Rx. 3 mo ago: SARS-CoV-2 mRNA vaccine.
CC: 2 mo on/off fever, cough, dyspnea. NP SARS-CoV-2 PCR neg. Rx as CAP w doxycycline - no response.
CT chest. DDx? Work up? #MayoIDQ next
42M on obinutuzumab for CLL. 4 mo ago: mild COVID-19 - no specific Rx. 3 mo ago: SARS-CoV-2 mRNA vaccine.
CC: 2 mo on/off fever, cough, dyspnea. NP SARS-CoV-2 PCR neg. Rx as CAP w doxycycline - no response.
CT chest. DDx? Work up? #MayoIDQ next

2/
Four months after mild COVID-19, an ICH man with CLL on obinutuzumab presents with prolonged / recurrent doxycycline-non responsive CAP. CT chest shown. See prior tweet for other details. Which of the following is the most likely diagnosis? #MayoIDQ
Four months after mild COVID-19, an ICH man with CLL on obinutuzumab presents with prolonged / recurrent doxycycline-non responsive CAP. CT chest shown. See prior tweet for other details. Which of the following is the most likely diagnosis? #MayoIDQ
3/
All of the MCQ choices could be possible in this case. Imaging suggested viral or PJP.
Work up:
Serum BDG / GM negative
CMV PCR negative
BAL PJP PCR negative
BAL SARS-CoV-2 PCR +++
SARS-CoV-2 spike/nucleocapsid Ab negative (despite infection / vaccine)
All of the MCQ choices could be possible in this case. Imaging suggested viral or PJP.
Work up:
Serum BDG / GM negative
CMV PCR negative
BAL PJP PCR negative
BAL SARS-CoV-2 PCR +++
SARS-CoV-2 spike/nucleocapsid Ab negative (despite infection / vaccine)
Images of Infectious Diseases
This is middle turbinate of a 64 ICH with epistaxis s/p CAR-T for refractory diffuse large B cell lymphoma.
What is your DDx? #MayoIDQ next
This is middle turbinate of a 64 ICH with epistaxis s/p CAR-T for refractory diffuse large B cell lymphoma.
What is your DDx? #MayoIDQ next

64M refractory DLBCL
s/p CAR-T —> cytokine release syndrome Rx tocilizumab and steroids
CC: epistaxis x 2w
PE: lesion in hard palate; nasal endoscopy (photo). CT dense material in sinuses.
What is next best step?
s/p CAR-T —> cytokine release syndrome Rx tocilizumab and steroids
CC: epistaxis x 2w
PE: lesion in hard palate; nasal endoscopy (photo). CT dense material in sinuses.
What is next best step?
3/
Biopsies from left hard palate and nasal cavity lesions were obtained (photo). Culture: Fusarium sp.
Suggested answer: ENT surgery for biopsy / diagnostics + debridement
Often: diagnostics and empiric Rx are concurrent in real life.
Biopsies from left hard palate and nasal cavity lesions were obtained (photo). Culture: Fusarium sp.
Suggested answer: ENT surgery for biopsy / diagnostics + debridement
Often: diagnostics and empiric Rx are concurrent in real life.

Images of Infectious Diseases
H&E of brain biopsy specimen.
Who is the host? What is the most likely pathogen? How do you treat?
#MayoIDQ
H&E of brain biopsy specimen.
Who is the host? What is the most likely pathogen? How do you treat?
#MayoIDQ

2/ #MayoIDQ
75F. Immunocompetent.
CC: headache x few months —> now left leg weakness, blurred vision, seizure. CBC/CMP normal. CT head: mass in right ventricle, pons. CT chest/abdomen for CA work up (-). Brain biopsy (photo).
Which of the following is the most likely pathogen?
75F. Immunocompetent.
CC: headache x few months —> now left leg weakness, blurred vision, seizure. CBC/CMP normal. CT head: mass in right ventricle, pons. CT chest/abdomen for CA work up (-). Brain biopsy (photo).
Which of the following is the most likely pathogen?
3/
Case diagnosis: cerebral #phaeohyphomycosis due to #cladophialophora
Note pigmented hyphae —> excludes Aspergillus (hyaline septate mould)
Among 3 remaining choices, the most common neurotrophic dematiaceous mould is Cladophialophora bantiana
Case diagnosis: cerebral #phaeohyphomycosis due to #cladophialophora
Note pigmented hyphae —> excludes Aspergillus (hyaline septate mould)
Among 3 remaining choices, the most common neurotrophic dematiaceous mould is Cladophialophora bantiana
#MayoIDQ #IDBR
45M CC: tender mass on left thigh that started as an “insect bite” 4 days ago. No F/C. PE: tender fluctuant 2-cm mass with surrounding erythema.
After I&D of abscess in the clinic, what do you recommend?
45M CC: tender mass on left thigh that started as an “insect bite” 4 days ago. No F/C. PE: tender fluctuant 2-cm mass with surrounding erythema.
After I&D of abscess in the clinic, what do you recommend?
2/
2014 IDSA guideline recommends incision and drainage of purulent SSTI (abscess)
Antibiotics vs MRSA / S. aureus as an adjunct to I&D if:
1. SIRS
2. Failed initial Ab Rx
3. Impaired host defense
Any new data since then?
doi.org/10.1093/cid/ci…
2014 IDSA guideline recommends incision and drainage of purulent SSTI (abscess)
Antibiotics vs MRSA / S. aureus as an adjunct to I&D if:
1. SIRS
2. Failed initial Ab Rx
3. Impaired host defense
Any new data since then?
doi.org/10.1093/cid/ci…
3/
After 2014 IDSA guideline, placebo-controlled RCTs were published on use of antibiotics (TMP SMX or clindamycin) for uncomplicated SSTI abscess ... (next)
ncbi.nlm.nih.gov/pmc/articles/P…
After 2014 IDSA guideline, placebo-controlled RCTs were published on use of antibiotics (TMP SMX or clindamycin) for uncomplicated SSTI abscess ... (next)
ncbi.nlm.nih.gov/pmc/articles/P…
#MayoIDQ: 86M DM
2 wk of R ear pain / nasal discharge
Now: R frontal HA, facial pain, vision loss
PE: R ptosis, CN III, IV, VI palsies, purulence R middle meatus
CT: R sided paranasal sinusitis w/ phlegmonous extension to orbital apex
What is DDx, work up and etiology?
2 wk of R ear pain / nasal discharge
Now: R frontal HA, facial pain, vision loss
PE: R ptosis, CN III, IV, VI palsies, purulence R middle meatus
CT: R sided paranasal sinusitis w/ phlegmonous extension to orbital apex
What is DDx, work up and etiology?
2/
Diagnosis: Orbital Apex Syndrome
S/S due to involvement of structures in orbital apex: most common vision loss and painful / limited eye movement
CN palsies
* Optic nerve
* Oculomotor nerve
* Trochlear nerve
* First division of trigeminal nerve
* Abducens nerve
Diagnosis: Orbital Apex Syndrome
S/S due to involvement of structures in orbital apex: most common vision loss and painful / limited eye movement
CN palsies
* Optic nerve
* Oculomotor nerve
* Trochlear nerve
* First division of trigeminal nerve
* Abducens nerve
3/
DDx (overlapping symptoms) of orbital apex syndrome
1. Cavernous sinus thrombosis
2. Superior orbital fissure syndrome
ncbi.nlm.nih.gov/pmc/articles/P…
DDx (overlapping symptoms) of orbital apex syndrome
1. Cavernous sinus thrombosis
2. Superior orbital fissure syndrome
ncbi.nlm.nih.gov/pmc/articles/P…
Images of Infectious Diseases
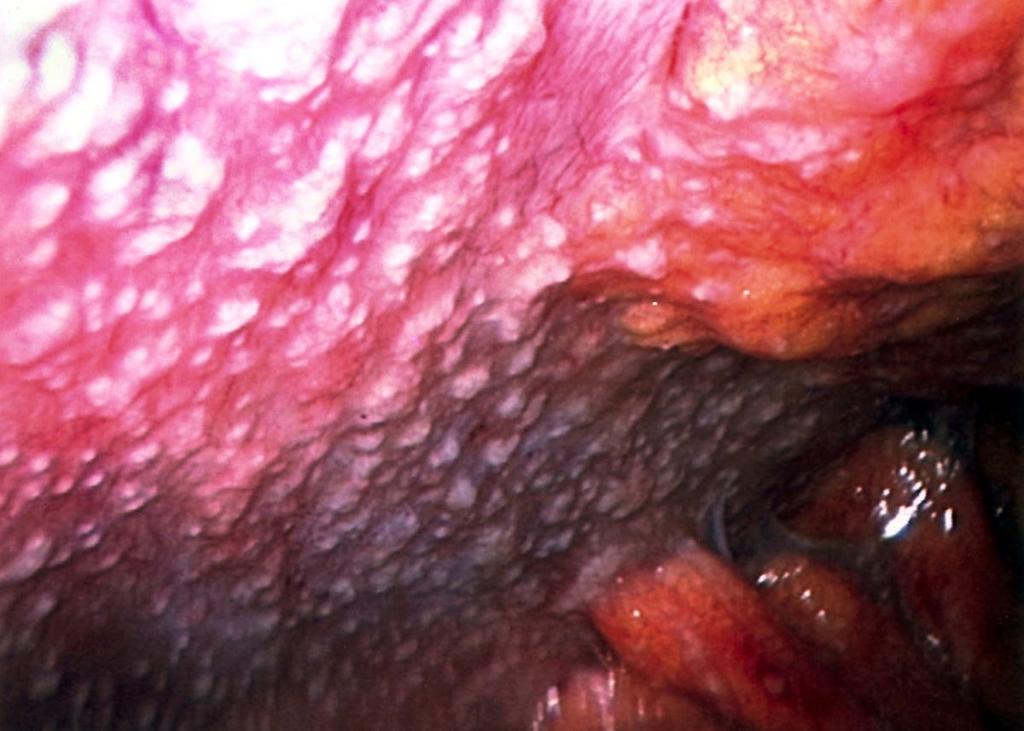
28F SLE on MTX
CC chest pain, vaginal DC
Rx pred for lupus
2 mo: fatigue, pruritic rash, visual floaters Rx pred
1 mo: blurred vision. PE iritis / chorioretinitis. Rx pred
Now b/l vision loss. PE panuveitis + chorioretinitis
DDx? #MayoIDQ
28F SLE on MTX
CC chest pain, vaginal DC
Rx pred for lupus
2 mo: fatigue, pruritic rash, visual floaters Rx pred
1 mo: blurred vision. PE iritis / chorioretinitis. Rx pred
Now b/l vision loss. PE panuveitis + chorioretinitis
DDx? #MayoIDQ

2/
28F HIV/HBV/HCV(-) SLE on MTX w chronic pain Rx as flare, vaginal discharge due to BV Rx metro (negative GC/chlamydia), skin rash x 2 w and progressive vision loss (photo). CXR clear. Indiana / no foreign travel. No animal exposures.
What is most likely diagnostic test?
28F HIV/HBV/HCV(-) SLE on MTX w chronic pain Rx as flare, vaginal discharge due to BV Rx metro (negative GC/chlamydia), skin rash x 2 w and progressive vision loss (photo). CXR clear. Indiana / no foreign travel. No animal exposures.
What is most likely diagnostic test?
3/
Case diagnosis: bilateral ocular syphilis with neurosyphilis
RPR 1:512
Syphilis antibody with reflex: positive
CSF VDRL 1:1
Rx: IV penicillin
Case diagnosis: bilateral ocular syphilis with neurosyphilis
RPR 1:512
Syphilis antibody with reflex: positive
CSF VDRL 1:1
Rx: IV penicillin
#MayoIDQ 69M was brought to the ED because of weakness. PE: intoxicated disheveled man with multiple skin ulcers / excoriations.
WBC 27. CK 1486. AST 76.
Wound culture: Clostridium botulinum
Which of the following is most consistent with wound botulism?
WBC 27. CK 1486. AST 76.
Wound culture: Clostridium botulinum
Which of the following is most consistent with wound botulism?
2/
#Botulism
#Botulinum neurotoxin binds to cholinergic nerve terminals and cleaves intracellular proteins needed for #acetylcholine release —> reduced acetylcholine —> neuromuscular blockade —> bulbar palsies, hypotonia, and symmetric, descending, #flaccid #paralysis.
#Botulism
#Botulinum neurotoxin binds to cholinergic nerve terminals and cleaves intracellular proteins needed for #acetylcholine release —> reduced acetylcholine —> neuromuscular blockade —> bulbar palsies, hypotonia, and symmetric, descending, #flaccid #paralysis.
3/
#Botulism
Clinical features
1. Flaccid paralysis
2. Prominent cranial nerve palsies
3. Descending progression
4. Symmetrical presentation
5. No sensory nerve dysfunction.
43% are correct in MCQ
cdc.gov/botulism/healt…
#Botulism
Clinical features
1. Flaccid paralysis
2. Prominent cranial nerve palsies
3. Descending progression
4. Symmetrical presentation
5. No sensory nerve dysfunction.
43% are correct in MCQ
cdc.gov/botulism/healt…
Weekend Digest
Name the pathogen!
H & E stain of heart tissue of a 27M who developed severe intractable heart failure 2 months after an allogeneic bone marrow transplant for acute leukemia.
Clue: consumption of food / water contaminated with feces of snakes
Name the pathogen!
H & E stain of heart tissue of a 27M who developed severe intractable heart failure 2 months after an allogeneic bone marrow transplant for acute leukemia.
Clue: consumption of food / water contaminated with feces of snakes

2/
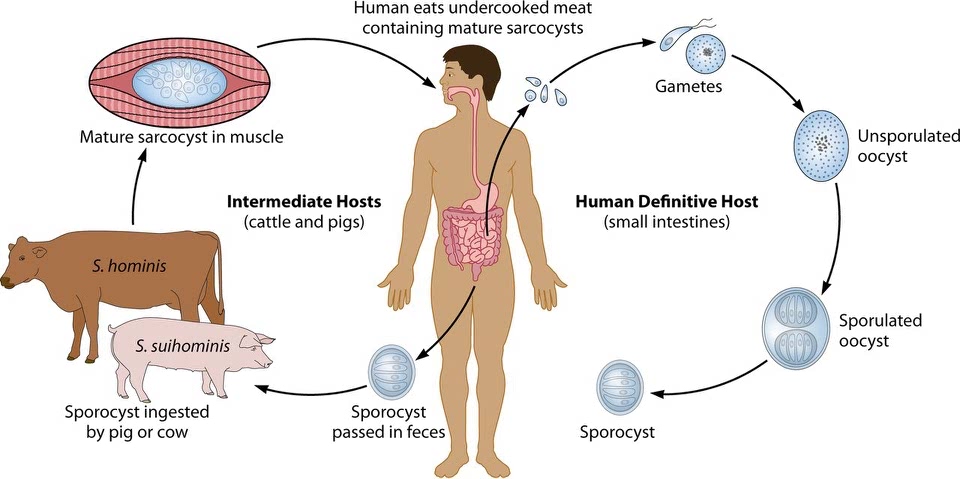
#Sarcocystosis
1. Sarcocystis hominis, suihominis, nesbetti, others
2. Zoonotic: 2 forms for human infection
3. Intestinal and muscular sarcosystosis
4. Dx: intestinal (O/P), muscular (biopsy)
5. Rx: not well defined; TMP-SMX, albendazole, others
cmr.asm.org/content/28/2/2…
#Sarcocystosis
1. Sarcocystis hominis, suihominis, nesbetti, others
2. Zoonotic: 2 forms for human infection
3. Intestinal and muscular sarcosystosis
4. Dx: intestinal (O/P), muscular (biopsy)
5. Rx: not well defined; TMP-SMX, albendazole, others
cmr.asm.org/content/28/2/2…
3/
Intestinal #Sarcocystosis
1. Ingestion of sarcocyst (S. hominis / beef, suihominis / pork) in tissue
2. Sarcocyst digested —> bradyzoites —> intestinal infection / gametes —> oocysts / sporocyst detected in stool
3. Self limited. No Rx needed
cmr.asm.org/content/28/2/2…
Intestinal #Sarcocystosis
1. Ingestion of sarcocyst (S. hominis / beef, suihominis / pork) in tissue
2. Sarcocyst digested —> bradyzoites —> intestinal infection / gametes —> oocysts / sporocyst detected in stool
3. Self limited. No Rx needed
cmr.asm.org/content/28/2/2…
Images of Infectious Diseases
GMS of sinus tissue of 20F with no PMH. She presented with fever and sinus pain. CT pansinusitis. Labs: WBC 1.7 ANC 0. Serum BDG and GM negative.
What is your differential diagnosis and empiric therapy? #MayoIDQ to follow...
GMS of sinus tissue of 20F with no PMH. She presented with fever and sinus pain. CT pansinusitis. Labs: WBC 1.7 ANC 0. Serum BDG and GM negative.
What is your differential diagnosis and empiric therapy? #MayoIDQ to follow...

2/
Histopath of surgically resected tissue shows fungal elements. You suggested Mucor/Rhizopus, Fusarium, Trichosporon.
Lack of serum BDG suggests Mucor/Rhizopus
The patient was started on AmBisome.
Few days later, the fungal culture of the same sinus sample shows (photo)
Histopath of surgically resected tissue shows fungal elements. You suggested Mucor/Rhizopus, Fusarium, Trichosporon.
Lack of serum BDG suggests Mucor/Rhizopus
The patient was started on AmBisome.
Few days later, the fungal culture of the same sinus sample shows (photo)

3/
#MayoIDQ Surgical debridement of the sinuses was performed plus liposomal Amphotericin B was initiated. Patient lives in rural MN and asks you if an oral option is available as step down Rx.
#MayoIDQ Surgical debridement of the sinuses was performed plus liposomal Amphotericin B was initiated. Patient lives in rural MN and asks you if an oral option is available as step down Rx.
Images of Infectious Diseases
6 mo post-tx: H&E (400x) of cervical biopsy of 46F s/p living unrelated donor kidney tx for adult PCKD.
Belatacept. MMF. Prednisone.
Acute cellular + antibody-mediated rejection.
CMV D+/R-. valganciclovir prophylaxis.
DDx / Rx? #MayoIDQ next
6 mo post-tx: H&E (400x) of cervical biopsy of 46F s/p living unrelated donor kidney tx for adult PCKD.
Belatacept. MMF. Prednisone.
Acute cellular + antibody-mediated rejection.
CMV D+/R-. valganciclovir prophylaxis.
DDx / Rx? #MayoIDQ next

2/
Case diagnosis: breakthrough CMV disease with cervicitis
H&E intranuclear / intracytoppasmic inclusions within endothelial cells in ectocervical stroma.
Immunohistochemistry stain for CMV shows infected endothelial cells with CMV inclusions.
doi.org/10.1111/tid.13…
Case diagnosis: breakthrough CMV disease with cervicitis
H&E intranuclear / intracytoppasmic inclusions within endothelial cells in ectocervical stroma.
Immunohistochemistry stain for CMV shows infected endothelial cells with CMV inclusions.
doi.org/10.1111/tid.13…

3/
#MayoIDQ Breakthrough CMV disease, while receiving valGCV prophylaxis, is concerning for over-immunosuppression, under-dosing of val GCV, and/or drug-resistant virus.
If gene sequencing shows the most common CMV gene mutation, what drug would be recommended Rx?
#MayoIDQ Breakthrough CMV disease, while receiving valGCV prophylaxis, is concerning for over-immunosuppression, under-dosing of val GCV, and/or drug-resistant virus.
If gene sequencing shows the most common CMV gene mutation, what drug would be recommended Rx?
Images of Infectious Diseases
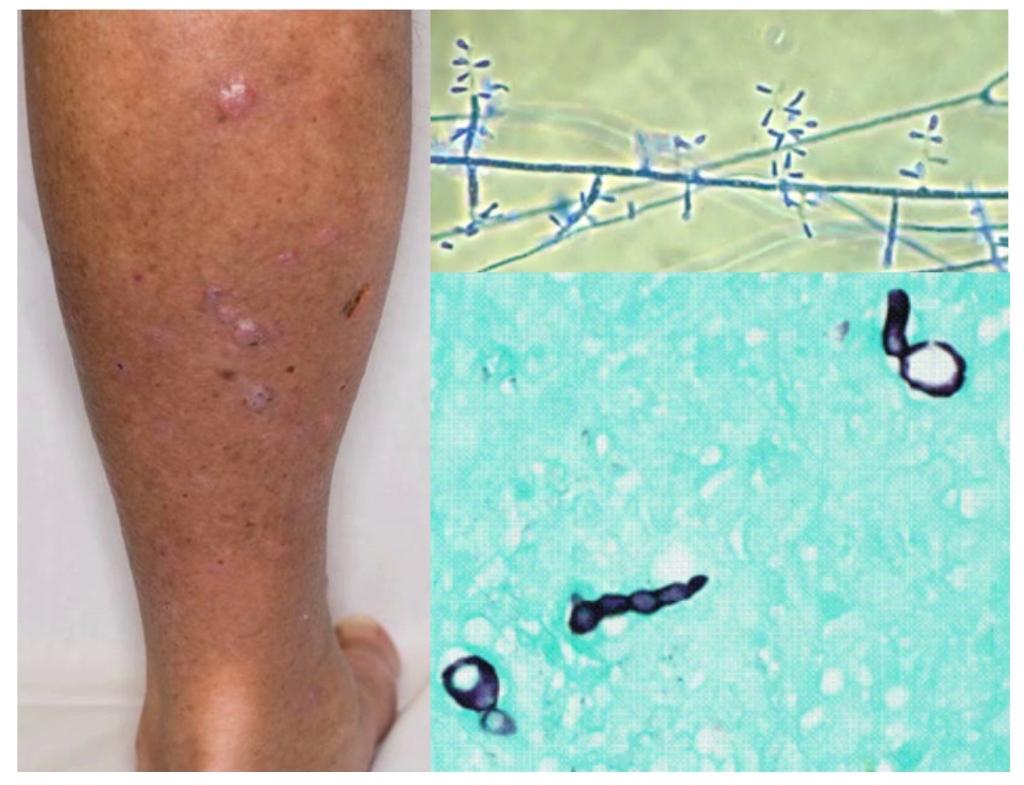
This is GMS stain and culture of a skin biopsy from a patient’s leg.
Who is the host? What is the syndrome? Name the pathogen. How to treat?
#MayoIDQ and case details to follow...
This is GMS stain and culture of a skin biopsy from a patient’s leg.
Who is the host? What is the syndrome? Name the pathogen. How to treat?
#MayoIDQ and case details to follow...
2/
66M. 4 mo after heart Tx: painless leg nodules that spread distally x 5 weeks. No pain. No fever.
PE unremarkable except lesions in left leg / foot + tinea pedis
Biopsy: GMS fungal elements in dermis. Culture: Trichophyton rubrum
What is true of this condition?
66M. 4 mo after heart Tx: painless leg nodules that spread distally x 5 weeks. No pain. No fever.
PE unremarkable except lesions in left leg / foot + tinea pedis
Biopsy: GMS fungal elements in dermis. Culture: Trichophyton rubrum
What is true of this condition?
3/
Case diagnosis:
#Majocchi’s Granuloma due to #Trichophyton rubrum
Histopath shows fungal elements (GMS) - not sufficient for identification.
Important: Send specimen for culture identification!!!
Treatment: Itraconazole Rx
Case diagnosis:
#Majocchi’s Granuloma due to #Trichophyton rubrum
Histopath shows fungal elements (GMS) - not sufficient for identification.
Important: Send specimen for culture identification!!!
Treatment: Itraconazole Rx
A series of images presented by an ID fellow to a faculty panel in the “Challenging Cases” session of the #MayoIDFellowsForum
The fellow asked the experts: What diagnosis comes to mind?
#IDTwitter, what do you think?
Clinical details, #MayoIDQ and MCQ to follow...
The fellow asked the experts: What diagnosis comes to mind?
#IDTwitter, what do you think?
Clinical details, #MayoIDQ and MCQ to follow...
2/
Awesome list of potential pathogens... from staphylococcus / streptococcus to nocardia, TB, fungi (Mucor, Candida, endemics) and toxoplasma, and others.
Without knowing the host and scenario, all are possible. Thank you #IDTwitter.
Now let us learn about the case details..
Awesome list of potential pathogens... from staphylococcus / streptococcus to nocardia, TB, fungi (Mucor, Candida, endemics) and toxoplasma, and others.
Without knowing the host and scenario, all are possible. Thank you #IDTwitter.
Now let us learn about the case details..
3/
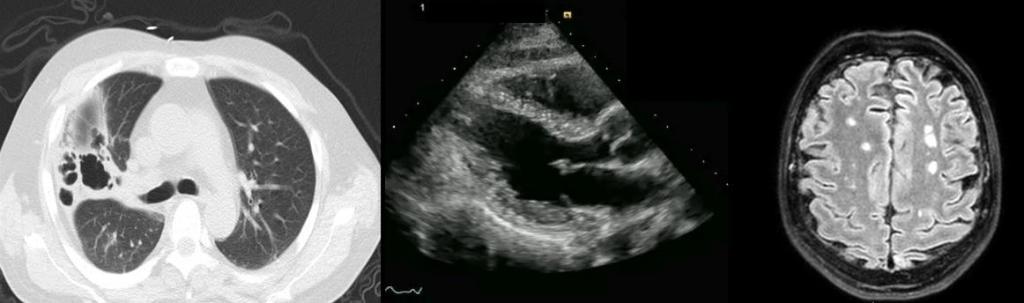
45M found unconscious.
PMH: alcohol use disorder. No IDU.
PE: T103F RR32 PR110
Meningismus.
Murmur. Rales.
No skin lesions.
WBC 27K.
Imaging (photo). No PFO.
CSF TNC 9450 /N92% /prot 150 / glu 20
Name the pathogen.
45M found unconscious.
PMH: alcohol use disorder. No IDU.
PE: T103F RR32 PR110
Meningismus.
Murmur. Rales.
No skin lesions.
WBC 27K.
Imaging (photo). No PFO.
CSF TNC 9450 /N92% /prot 150 / glu 20
Name the pathogen.
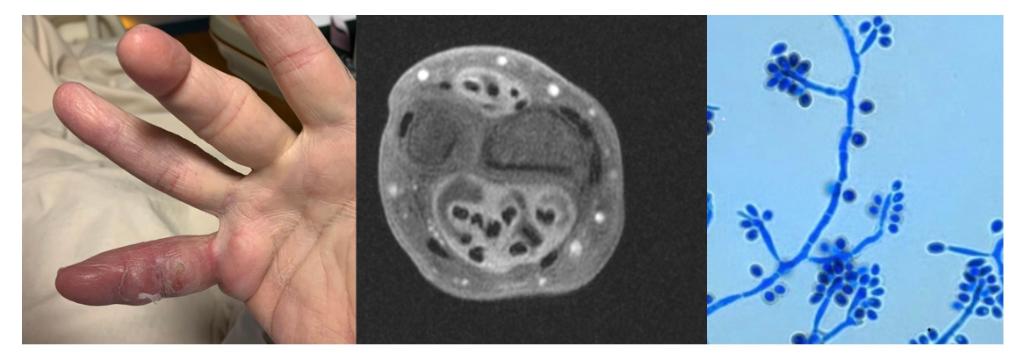
70M with swollen R 5th digit, hand and forearm. No fever / chills.
MRI: complex multi-compartment fluid collection with extensive flexor and extensor tenosynovitis
Debridement. Culture (photo).
What is your diagnosis and Rx?
#MayoIDQ MCQ to follow...
MRI: complex multi-compartment fluid collection with extensive flexor and extensor tenosynovitis
Debridement. Culture (photo).
What is your diagnosis and Rx?
#MayoIDQ MCQ to follow...
Elderly man with swollen right hand and forearm. MRI: complex fluid collection, extensive tenosynovitis. Debridement performed. Culture is shown (photo prior tweet).
Which of the following is the exposure associated with this infection?
Which of the following is the exposure associated with this infection?
3/
Beaver dam and blastomyces
When #IDBR says #beaverdam - you think #BLASTOMYCOSIS
nejm.org/doi/10.1056/NE…
Beaver dam and blastomyces
When #IDBR says #beaverdam - you think #BLASTOMYCOSIS
nejm.org/doi/10.1056/NE…
Images of Infectious Diseases
This is the histopath and gram stain of culture of a lymph node biopsy of a person with tender purulent inguinal adenopathy.
Dr. @dwchallener
Dr. @ali_eberly
MCQ #MayoIDQ to follow
This is the histopath and gram stain of culture of a lymph node biopsy of a person with tender purulent inguinal adenopathy.
Dr. @dwchallener
Dr. @ali_eberly
MCQ #MayoIDQ to follow
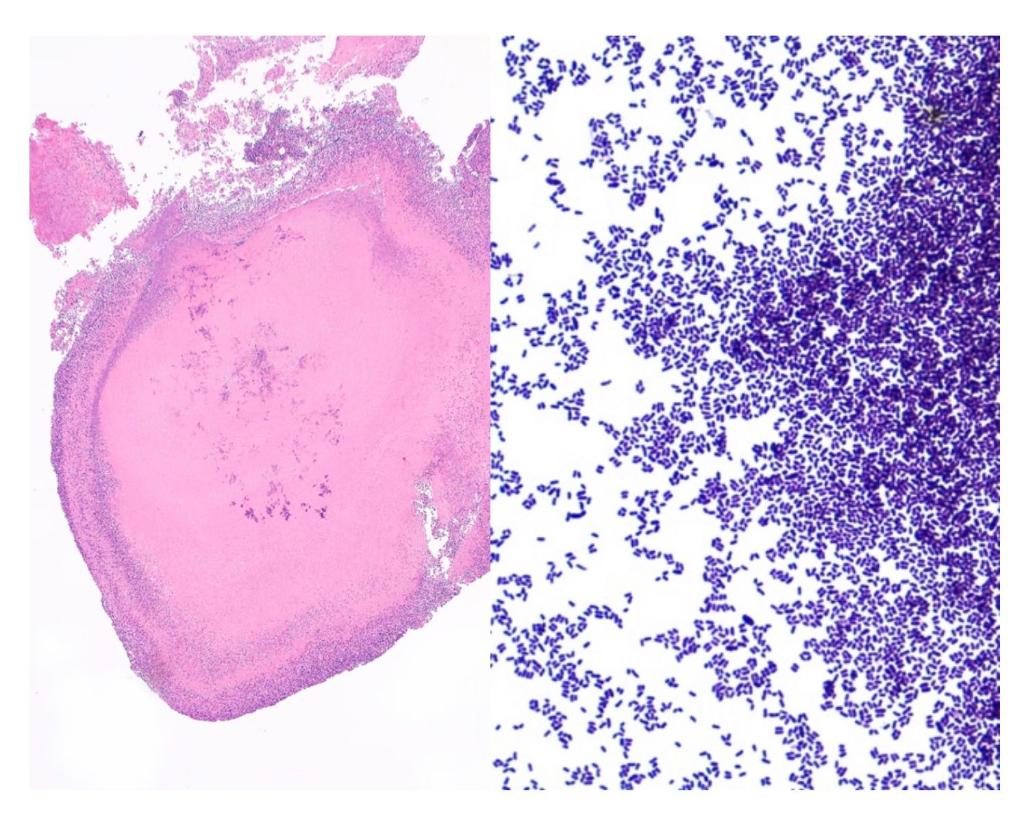
72M. Crohn’s. 2 pet dogs. 1 pet cat.
2 mo after L knee surgery —> tender L inguinal node with purulence. No F/C. No response to TMP-SMX.
Biopsy (see photo): Stellate suppurative granuloma with central necrosis and clumps of bacteria.
What is the most likely diagnosis?
2 mo after L knee surgery —> tender L inguinal node with purulence. No F/C. No response to TMP-SMX.
Biopsy (see photo): Stellate suppurative granuloma with central necrosis and clumps of bacteria.
What is the most likely diagnosis?
1/
#Gram stain: a first step in bacterial identification —> two major groups:
1. Gram-positive: retains primary stain (crystal violet)
2. Gram-negative: does not retain crystal violet but counterstained by safranin/fuchsine —> red / pink
Named after Hans Christian Gram (photo)
#Gram stain: a first step in bacterial identification —> two major groups:
1. Gram-positive: retains primary stain (crystal violet)
2. Gram-negative: does not retain crystal violet but counterstained by safranin/fuchsine —> red / pink
Named after Hans Christian Gram (photo)
On day 14 of neutropenia, an astute ID fellow noted this finding (photo) while examining a patient with fever. Underlying AML and ongoing chemotherapy.
What do you suspect? What work up do you suggest? Details and #MayoIDQ MCQ to follow...
What do you suspect? What work up do you suggest? Details and #MayoIDQ MCQ to follow...

65M acute myeloid leukemia. Rx: CLAG-M. Prophy ACV, posaconazole, Levo, inhaled pentamidine
D14 neutropenia: fever / chills
Exam: onychomycosis, rapidly evolving lesions in arms and torso (photo)
You asked for skin biopsy. Blood culture will grow what fungus?
D14 neutropenia: fever / chills
Exam: onychomycosis, rapidly evolving lesions in arms and torso (photo)
You asked for skin biopsy. Blood culture will grow what fungus?
2/
Case diagnosis: disseminated fusariosis
Majority got the diagnosis correctly!
Blood culture: Fusarium sp.
Rx: AmBisome / voriconazole
Hope for neutrophil recovery!!!
Case diagnosis: disseminated fusariosis
Majority got the diagnosis correctly!
Blood culture: Fusarium sp.
Rx: AmBisome / voriconazole
Hope for neutrophil recovery!!!
Images of Infectious Diseases
56M Mexico. Chronic abdominal pain, weight loss, anorexia.
Work up: elevated markers (CA19-9, CA-125, AFP). CXR normal. CT peritoneal carcinomatosis.
Laparoscopy (photo). Biopsy showed granuloma. What is your DDx? #MayoIDQ MCQ next...
56M Mexico. Chronic abdominal pain, weight loss, anorexia.
Work up: elevated markers (CA19-9, CA-125, AFP). CXR normal. CT peritoneal carcinomatosis.
Laparoscopy (photo). Biopsy showed granuloma. What is your DDx? #MayoIDQ MCQ next...
#MayoIDQ
Thank you for your responses.
Culture of tissue (peritoneal nodules) of this 56M (see prior tweet) with granuloma on biopsy: Mycobacterium tuberculosis complex. Resistant to pyrazinamide.
Which of these choices is the most likely mechanism of transmission?
Thank you for your responses.
Culture of tissue (peritoneal nodules) of this 56M (see prior tweet) with granuloma on biopsy: Mycobacterium tuberculosis complex. Resistant to pyrazinamide.
Which of these choices is the most likely mechanism of transmission?
1/
Case diagnosis: Peritoneal #tuberculosis due to #Mycobacterium #bovis
Path: granuloma and positive #AFB stain
Culture: M tuberculosis complex
Clue: #PZA resistance —> THINK M. bovis
Reported by @GaboMotoa during his rotation in Mayo Clinic
doi.org/10.1002/ccr3.3…
Case diagnosis: Peritoneal #tuberculosis due to #Mycobacterium #bovis
Path: granuloma and positive #AFB stain
Culture: M tuberculosis complex
Clue: #PZA resistance —> THINK M. bovis
Reported by @GaboMotoa during his rotation in Mayo Clinic
doi.org/10.1002/ccr3.3…
Images of Infectious Diseases
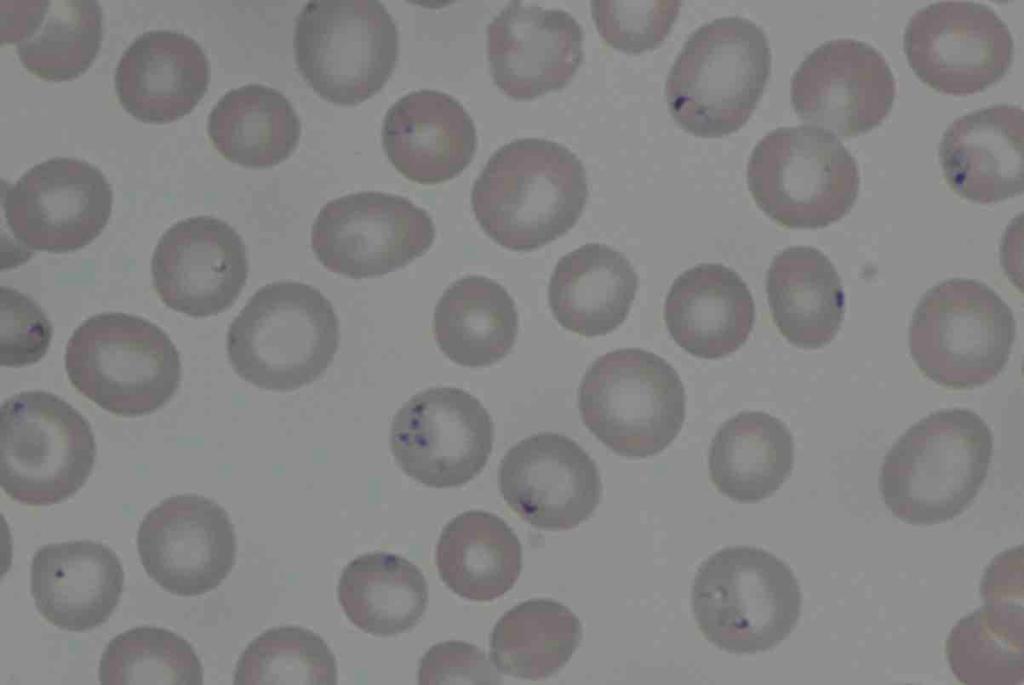
This is the peripheral blood smear of a 71M s/p splenectomy. Rural Wisconsin. No travel.
CC: fever, sweats, dyspnea
ROS: dark urine
PE: jaundice
Hgb 10. Low haptoglobin.
TBI 3.3 LDH 1075
What is the diagnosis and recommended Rx?
#MayoIDQ MCQ next
This is the peripheral blood smear of a 71M s/p splenectomy. Rural Wisconsin. No travel.
CC: fever, sweats, dyspnea
ROS: dark urine
PE: jaundice
Hgb 10. Low haptoglobin.
TBI 3.3 LDH 1075
What is the diagnosis and recommended Rx?
#MayoIDQ MCQ next
1/
71M. WI. (see prior tweet)
S/p splenectomy.
Fever, jaundice, hemolytic anemia.
Your diagnosis: babesiosis (parasitemia 7.3%).
3 days after starting Rx: tinnitus and hypoacusis
What Rx most likely caused this adverse effect?
71M. WI. (see prior tweet)
S/p splenectomy.
Fever, jaundice, hemolytic anemia.
Your diagnosis: babesiosis (parasitemia 7.3%).
3 days after starting Rx: tinnitus and hypoacusis
What Rx most likely caused this adverse effect?
2/
Treatment of #Babesiosis
1. Atovaquone-azithromycin
2. Quinine-clindamycin
The two regimens have comparable efficacy in non-life-threatening babesiosis.
BUT safety profile of Atovaquone-azithromycin was better
nejm.org/doi/full/10.10…
Treatment of #Babesiosis
1. Atovaquone-azithromycin
2. Quinine-clindamycin
The two regimens have comparable efficacy in non-life-threatening babesiosis.
BUT safety profile of Atovaquone-azithromycin was better
nejm.org/doi/full/10.10…
There is no proven effective antiviral drug for the treatment of #SARSCoV2
Several compounds are suggested for Rx of #COVID19. Based on the available in vitro and clinical data, which one is your preferred Rx, if available? #MayoIDQ references follow...
Several compounds are suggested for Rx of #COVID19. Based on the available in vitro and clinical data, which one is your preferred Rx, if available? #MayoIDQ references follow...
1/
#Chloroquine
Anti-malaria
Several potential mechanisms: change in cell membrane pH, impairs viral fusion, interferes with glycosylation of viral proteins
#chloroquine and #redemsivir are active against SARS-COV2 in experimental models
doi.org/10.1038/s41422…
#Chloroquine
Anti-malaria
Several potential mechanisms: change in cell membrane pH, impairs viral fusion, interferes with glycosylation of viral proteins
#chloroquine and #redemsivir are active against SARS-COV2 in experimental models
doi.org/10.1038/s41422…
2/
#Hydroxychloroquine
- Analogue of chloroquine
- Anti inflammatory effect
Hydroxychloroquine was more potent than chloroquine against #SARS-CoV2 in vitro.
doi.org/10.1093/cid/ci…
#Hydroxychloroquine
- Analogue of chloroquine
- Anti inflammatory effect
Hydroxychloroquine was more potent than chloroquine against #SARS-CoV2 in vitro.
doi.org/10.1093/cid/ci…
