
We provide psychiatry education for Psychiatrists, GPs & Mental Health Practitioners.
•
Join The Academy 👇
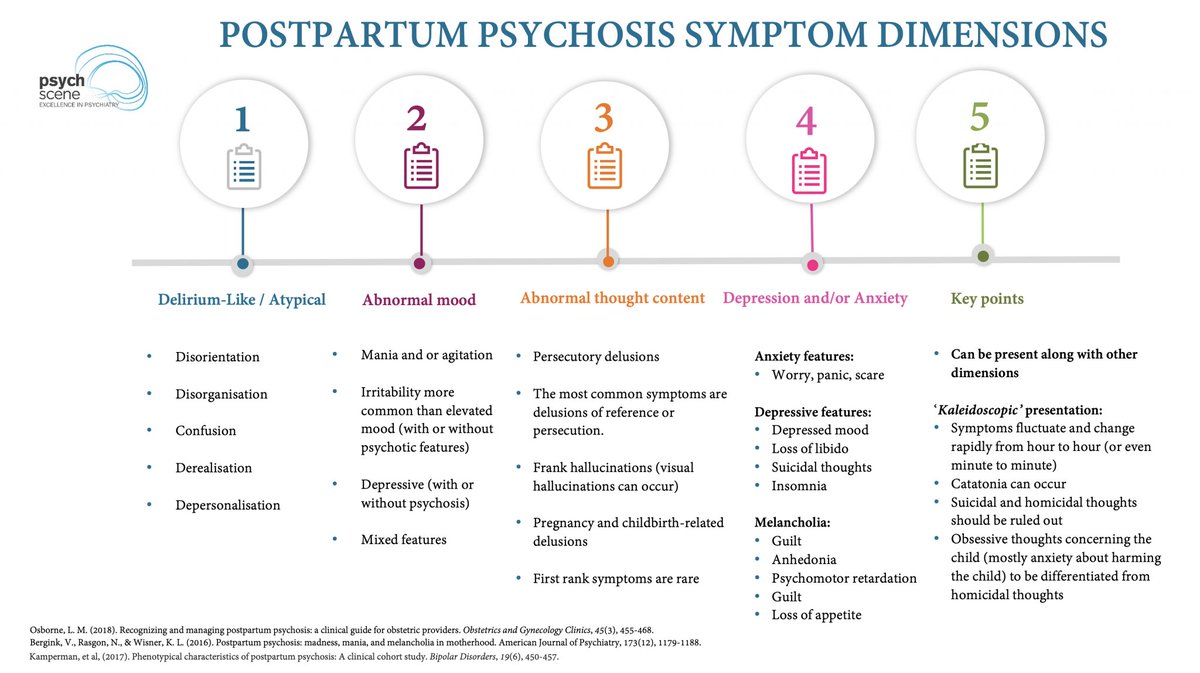 What is Postpartum Psychosis?
What is Postpartum Psychosis?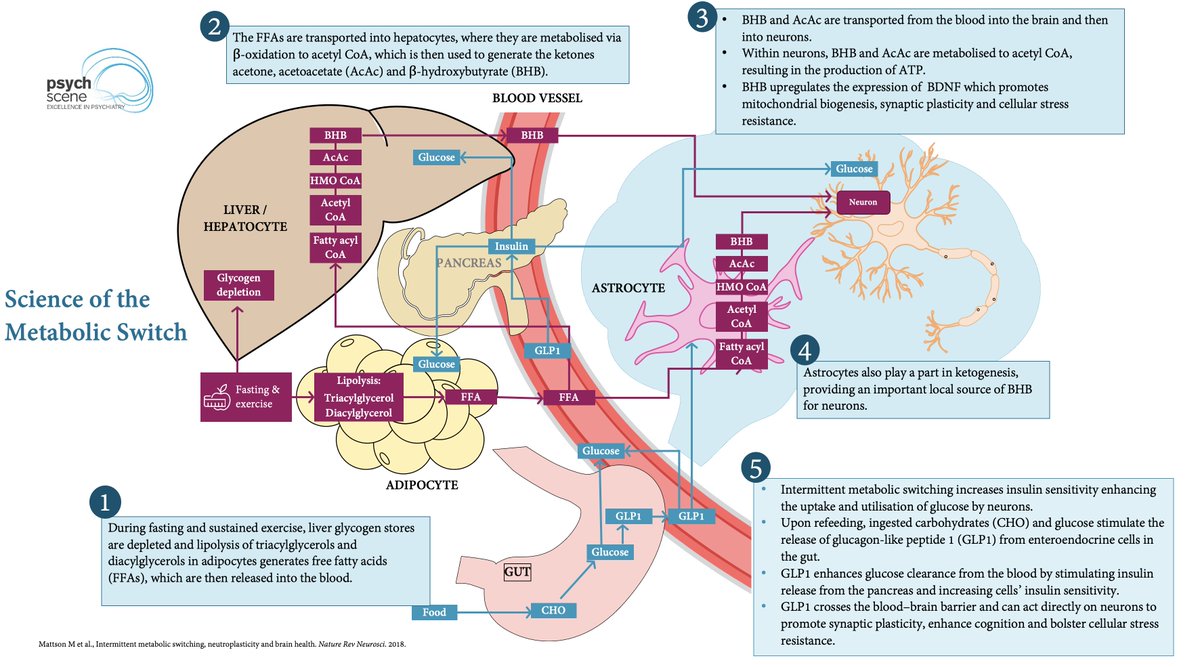 The Science Of The Metabolic Switch
The Science Of The Metabolic Switch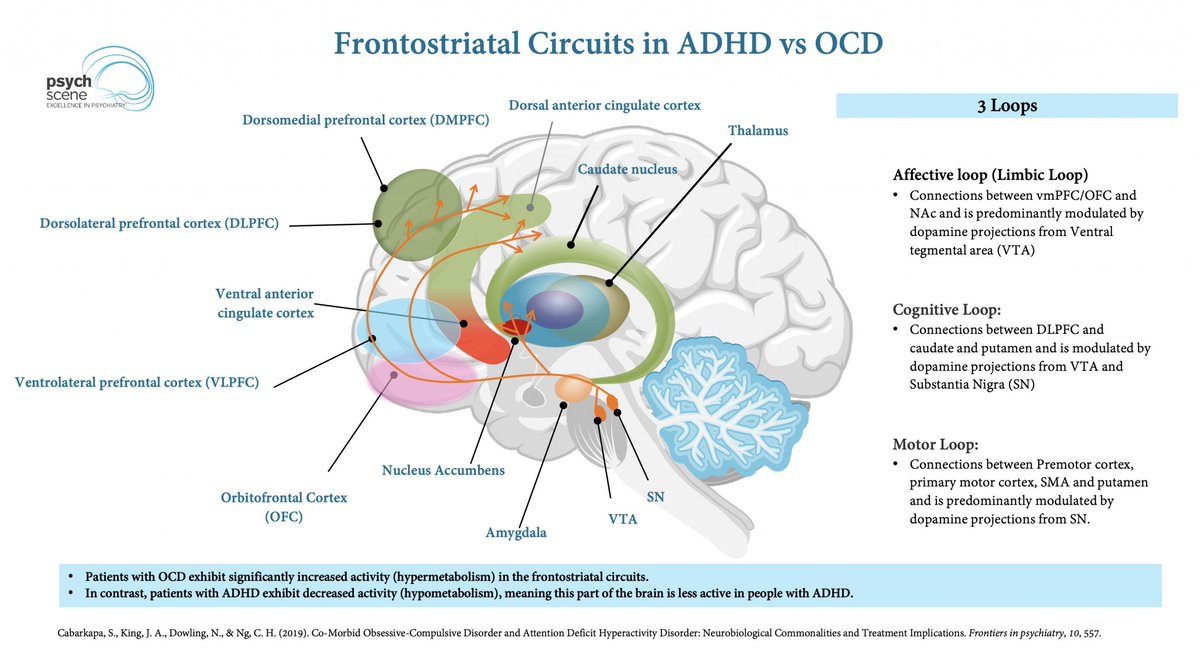 ADHD vs OCD
ADHD vs OCD For response rates (≥50% symptom reduction), these were the top performers:
For response rates (≥50% symptom reduction), these were the top performers: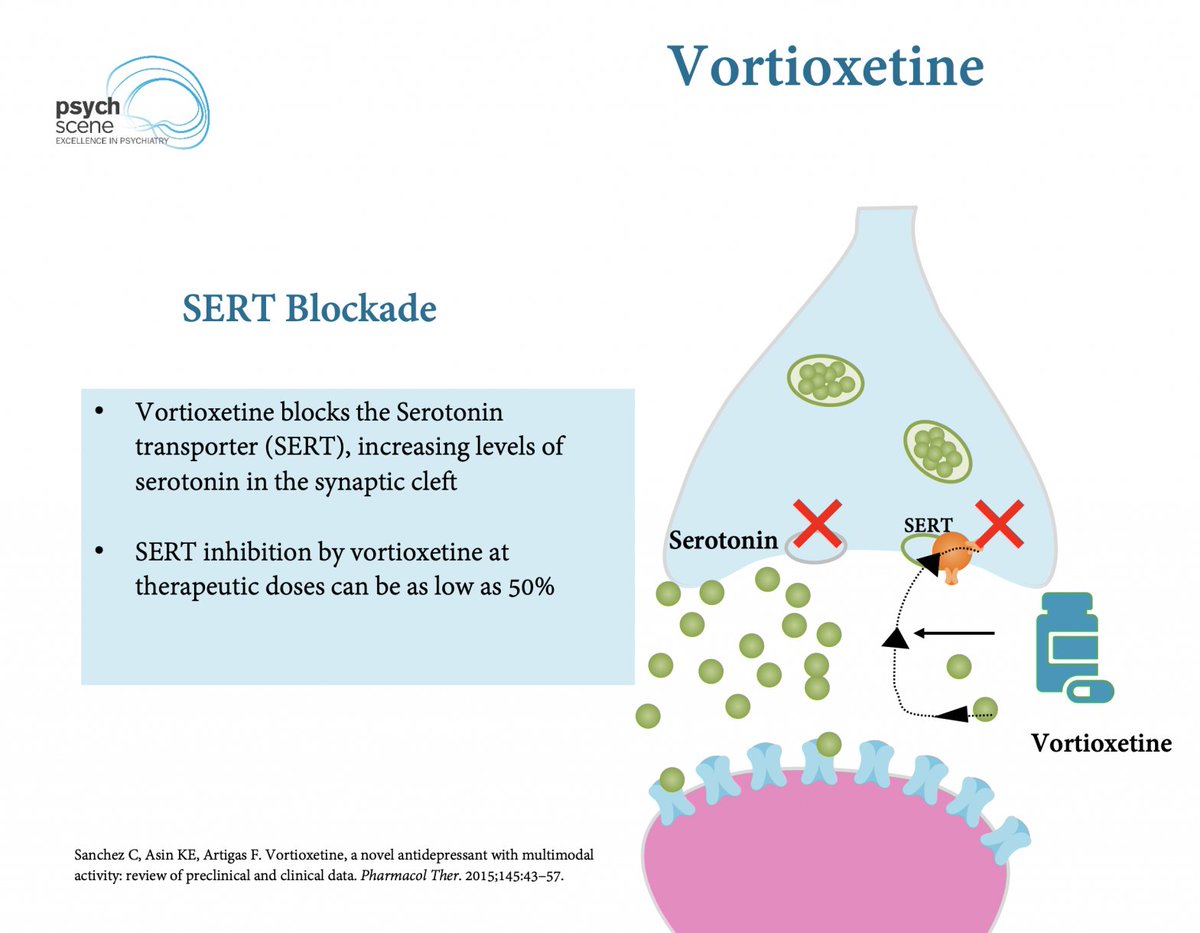 Pharmacological Profile & Multimodal Mechanism
Pharmacological Profile & Multimodal Mechanism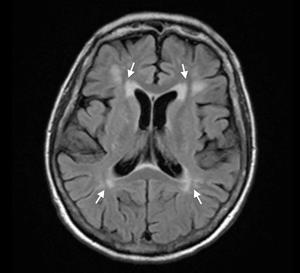 Full Symptom Profile
Full Symptom Profile Stress as a Cardiovascular Risk Factor
Stress as a Cardiovascular Risk Factor Two PTSD Phenotypes
Two PTSD Phenotypes
 Neurobiology of Nicotine Dependence
Neurobiology of Nicotine Dependence The Scope of the Problem
The Scope of the Problem CB1 & CB2 Receptors
CB1 & CB2 Receptors What are Reward Prediction Errors (RPEs)?
What are Reward Prediction Errors (RPEs)? The Triple Network Model
The Triple Network Model
 Why Does Memantine Matter?
Why Does Memantine Matter? 1️⃣ Understanding QTc Prolongation & TdP Risk
1️⃣ Understanding QTc Prolongation & TdP Risk Recognising Key Symptoms of Generalised Anxiety Disorder (GAD)
Recognising Key Symptoms of Generalised Anxiety Disorder (GAD)
 What is Anti-NMDAR Encephalitis?
What is Anti-NMDAR Encephalitis?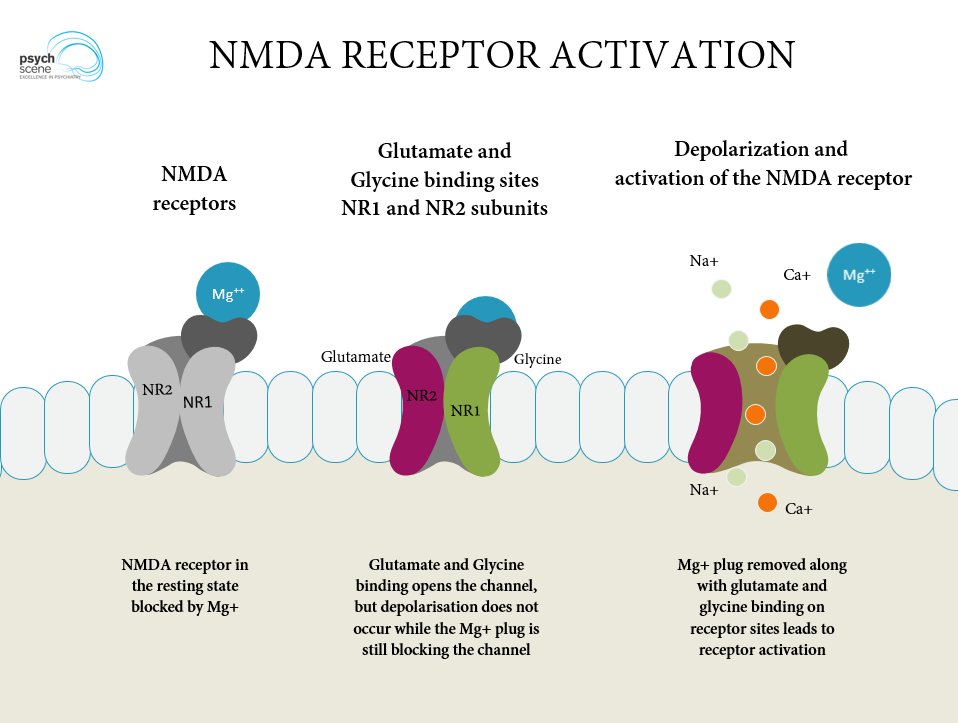
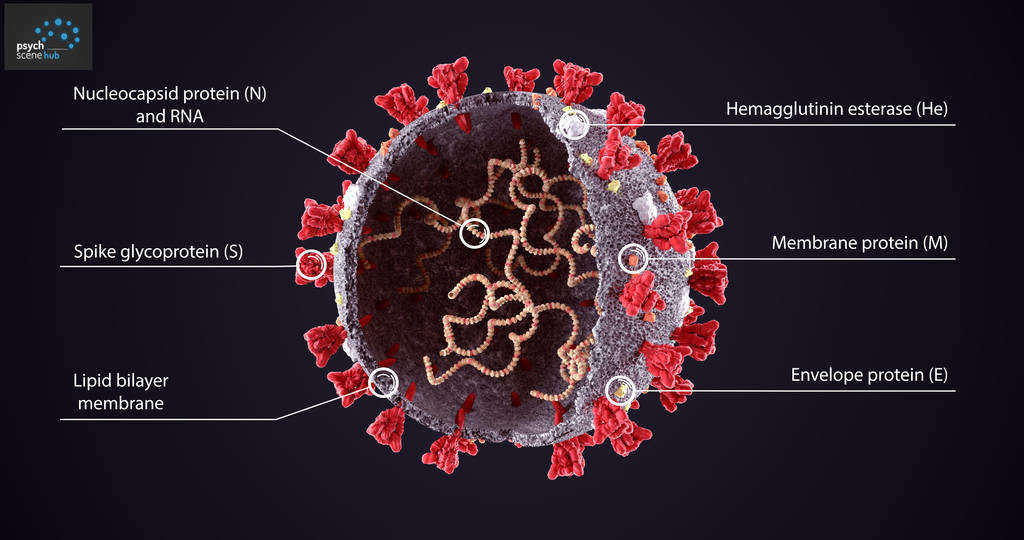 How does SARS-CoV-2 'invade' the CNS (central nervous system)?
How does SARS-CoV-2 'invade' the CNS (central nervous system)?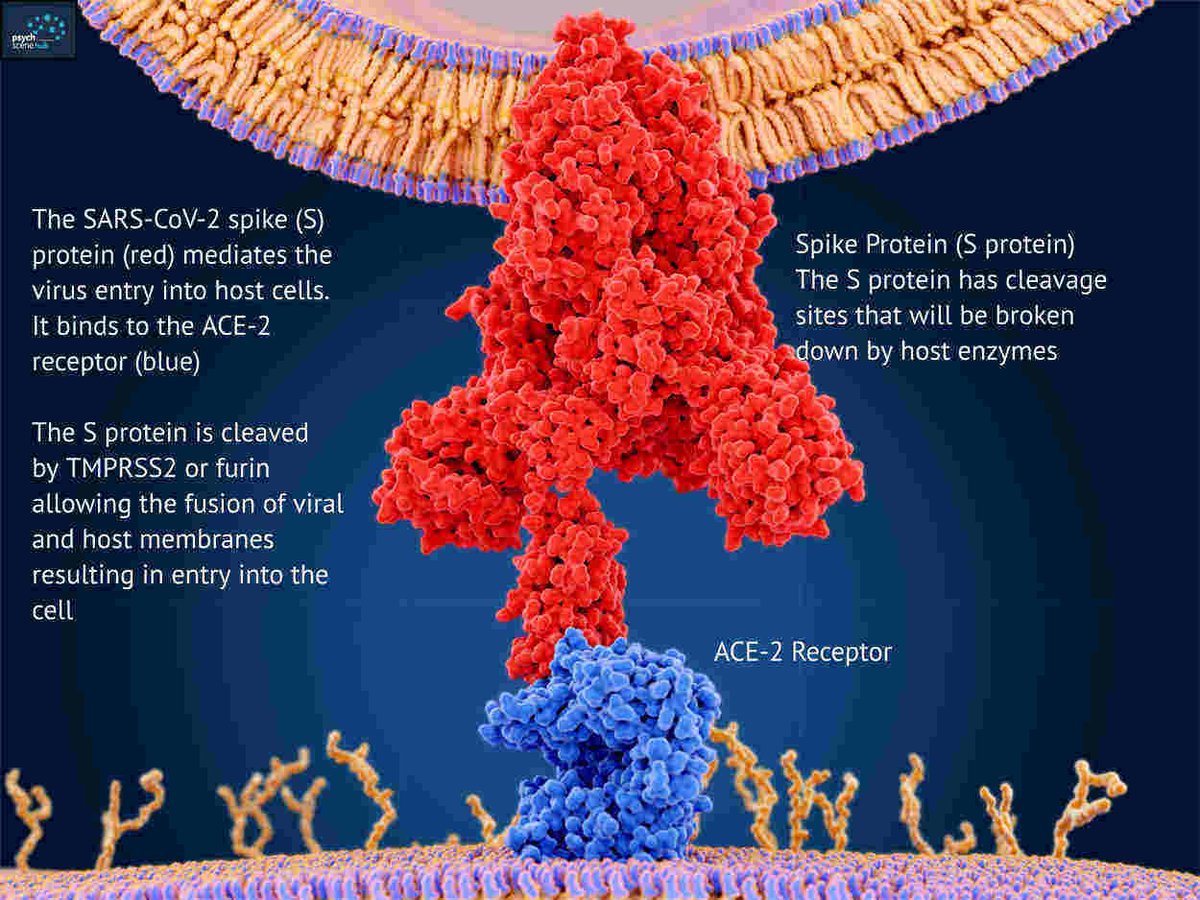
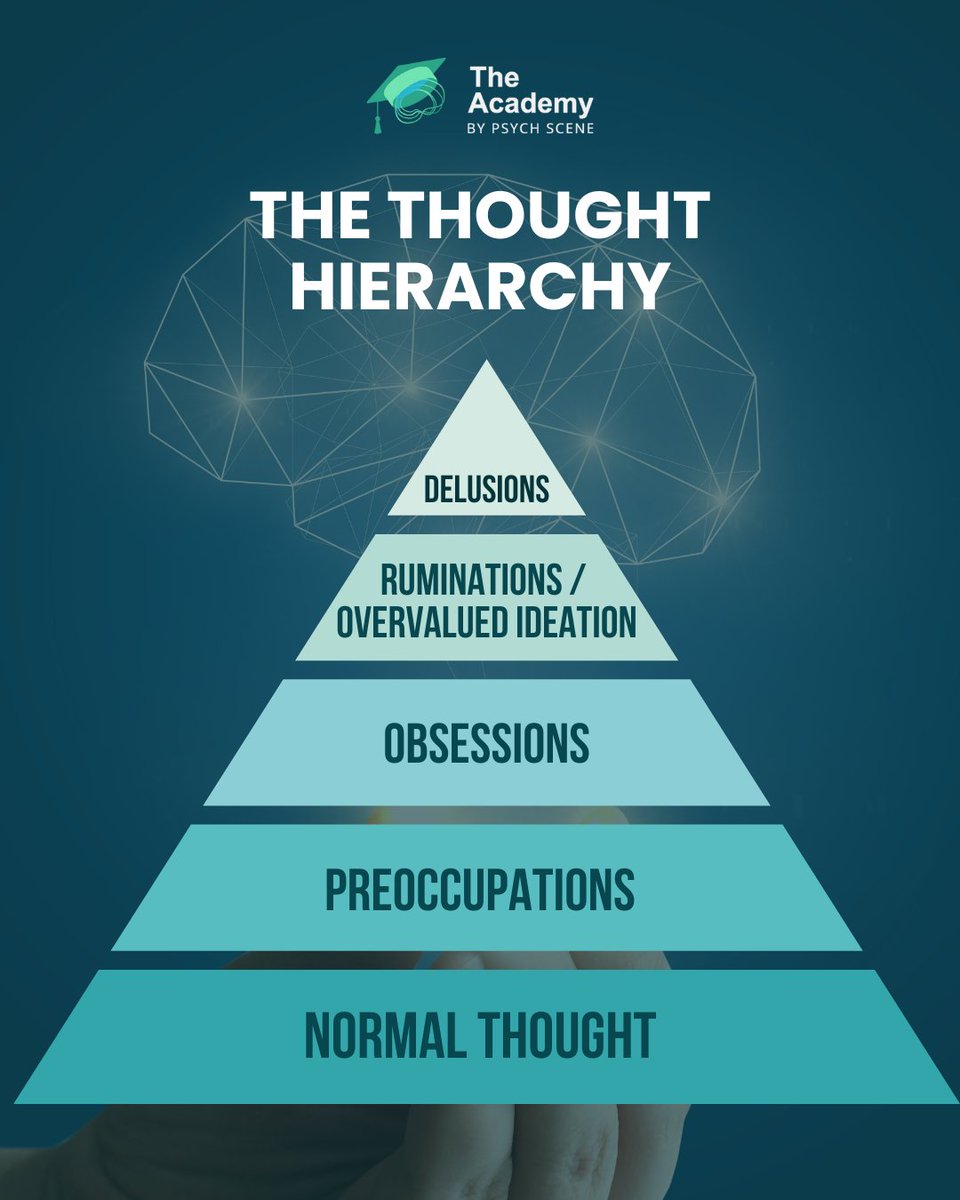 Thoughts are shaped by salience—our mind’s ability to prioritise stimuli.
Thoughts are shaped by salience—our mind’s ability to prioritise stimuli.