Discover and read the best of Twitter Threads about #morningreport
Most recents (16)

1/6
#Morningreport recently @SinaiBmoreIMRes
featured an interesting case by Paul Stendahl Dy
A young pt presenting with right sided CP, dyspnea s/p MVA and recent dx of necrotizing PNA,
DDx ???
#MedTwitter #Medstudenttwitter @SinaiChiefs
#Morningreport recently @SinaiBmoreIMRes
featured an interesting case by Paul Stendahl Dy
A young pt presenting with right sided CP, dyspnea s/p MVA and recent dx of necrotizing PNA,
DDx ???
#MedTwitter #Medstudenttwitter @SinaiChiefs

2/6
Vital signs:
T 37.8 P 117 BP 125/71 SPO2 94 % on RA
Exam:
Chest- decreased BS right lower side.
WBC: 15
Vital signs:
T 37.8 P 117 BP 125/71 SPO2 94 % on RA
Exam:
Chest- decreased BS right lower side.
WBC: 15

3/6 Imaging:
CXR: (image from internet)
CXR: (image from internet)

1/9
#Morningreport this week @SinaiBmoreIMRes
featured an interesting case by N. walia
A young Pt presenting with pancreatitis - develops complaints of "bilateral vision loss with progressively worsening headaches "
DDx ???
#MedTwitter #Medstudenttwitter
#Morningreport this week @SinaiBmoreIMRes
featured an interesting case by N. walia
A young Pt presenting with pancreatitis - develops complaints of "bilateral vision loss with progressively worsening headaches "
DDx ???
#MedTwitter #Medstudenttwitter

2/9
BP noted to be: BP: 207/117
Exam:
Eyes: EOMI.
Cannot count fingers.
Appreciates some movement on the right which appear as shadows.
Unable to detect static objects
Neuro: Exam normal
BP noted to be: BP: 207/117
Exam:
Eyes: EOMI.
Cannot count fingers.
Appreciates some movement on the right which appear as shadows.
Unable to detect static objects
Neuro: Exam normal
3/9
DDx: Vision loss/Headache ??
Giant Cell Arteritis (GCA)
Migraine
Retinal migraine
Hypertensive retinopathy
optic neuritis
Cerebral venous sinus thrombosis
Intracranial hemorrhage
Posterior circulation stroke
Primary CNS vasculitis
etc
DDx: Vision loss/Headache ??
Giant Cell Arteritis (GCA)
Migraine
Retinal migraine
Hypertensive retinopathy
optic neuritis
Cerebral venous sinus thrombosis
Intracranial hemorrhage
Posterior circulation stroke
Primary CNS vasculitis
etc

#ICYMI, CMR @HelyShahMD took us through a case of nephrotic syndrome last week and explored the various complications of nephrotic syndrome based on what protein is lost in the urine. Here’s a quick review of some of her teaching points!
#MedTwitter #MorningReport
#MedTwitter #MorningReport
1/
1️⃣ Spot urine protein/creatinine ratio correlates well with 24hr urine collection (except for patients with high protein excretion). Easier to collect than 24hr urine!
2️⃣ Urine specific gravity can falsely over- or underestimate proteinuria
pubmed.ncbi.nlm.nih.gov/16756640/
1️⃣ Spot urine protein/creatinine ratio correlates well with 24hr urine collection (except for patients with high protein excretion). Easier to collect than 24hr urine!
2️⃣ Urine specific gravity can falsely over- or underestimate proteinuria
pubmed.ncbi.nlm.nih.gov/16756640/
2/
3️⃣ Nephrotic syndrome is associated with several complications based on what protein is lost in the urine (some impromptu whiteboard teaching from the residents seen here!)
Here are four of these complications:
3️⃣ Nephrotic syndrome is associated with several complications based on what protein is lost in the urine (some impromptu whiteboard teaching from the residents seen here!)
Here are four of these complications:

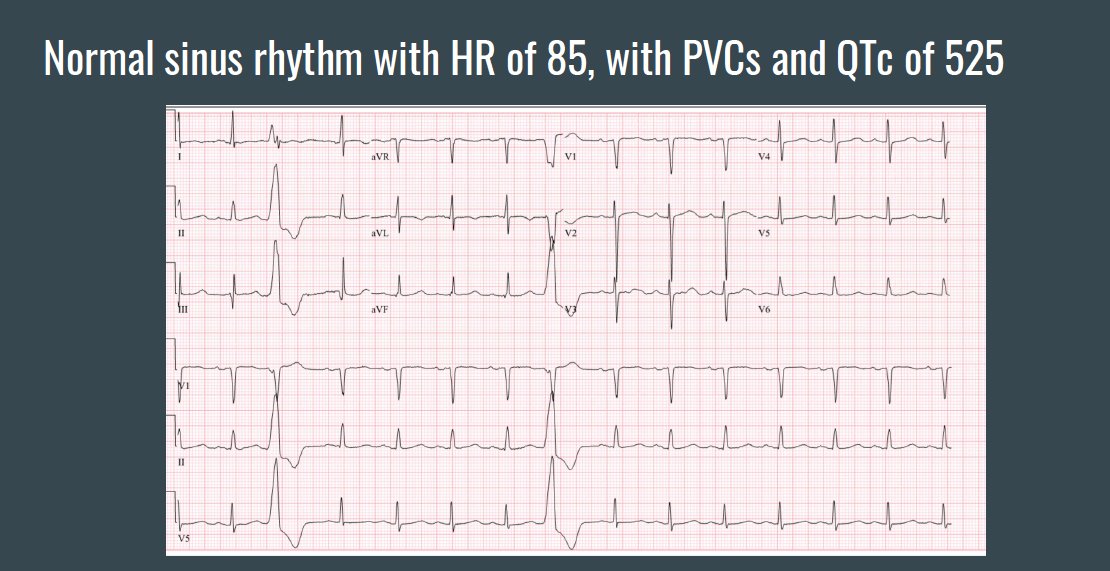
1/9 #Morningreport recently @SinaiBmoreIMRes
by M. Thomas featured a middle aged pt presenting with sudden collapse whilst getting ready in the morning.
No prodromal episodes
#DDx ?
#MedTwitter #MedStudentTwitter #FOAMed
by M. Thomas featured a middle aged pt presenting with sudden collapse whilst getting ready in the morning.
No prodromal episodes
#DDx ?
#MedTwitter #MedStudentTwitter #FOAMed

2/9
For acute collapse, this would need to be defined along the spectrum of:
Pre-syncope-> Syncope-> Near SCD-> SCD.
For acute collapse, this would need to be defined along the spectrum of:
Pre-syncope-> Syncope-> Near SCD-> SCD.

3/9
A quick review of medications show multiple medications that can present with this condition:
A quick review of medications show multiple medications that can present with this condition:
1/10 #Morningreport recently
@SinaiBmoreIMRes by S. Sridhar recently featured a pt with a 3 week history of generalized pruritic rash
#DDx ?
#MedTwitter #MedStudentTwitter #FOAMed
@SinaiBmoreIMRes by S. Sridhar recently featured a pt with a 3 week history of generalized pruritic rash
#DDx ?
#MedTwitter #MedStudentTwitter #FOAMed

2/10 The rash was insidious in onset, initially involving extremities and progressed to involve rest of the body, sparing face, palms, and soles.
Reports ~40 lb unintentional weight loss in previous 4-5 months.
Ddx for this rash would be :
emedicalhub.com/maculopapular-…
Reports ~40 lb unintentional weight loss in previous 4-5 months.
Ddx for this rash would be :
emedicalhub.com/maculopapular-…

3/10
Vital Signs: T-36.2, HR-92, RR-16, BP-109/75
Physical Exam:
Diffuse, erythematous, macular rash involving majority of bilateral upper and lower extremities, anterior and posterior trunk and abdomen.
Left occipital LN 1cm +. Rest of the examination was normal
Vital Signs: T-36.2, HR-92, RR-16, BP-109/75
Physical Exam:
Diffuse, erythematous, macular rash involving majority of bilateral upper and lower extremities, anterior and posterior trunk and abdomen.
Left occipital LN 1cm +. Rest of the examination was normal
1/10 #Morningreport recently @SinaiBmoreIMRes
by N.Rapista recently featured an elderly pt with an episode of dysphagia x 1 week
#DDx ?
#MedTwitter #MedStudentTwitter #FOAMed
by N.Rapista recently featured an elderly pt with an episode of dysphagia x 1 week
#DDx ?
#MedTwitter #MedStudentTwitter #FOAMed

2/10 Further history:
Unable to swallow any solid food
• “held in the throat”
• coughing frequently
• Generalized malaise
• New left ptosis
Unable to swallow any solid food
• “held in the throat”
• coughing frequently
• Generalized malaise
• New left ptosis
3/10EXAM:
T: 36.4°C BP: 139/69 HR: 68 RR: 18 SpO2: 100% on room air
Gen: Awake, alert
HENT: Left ptosis
Neuro: A&Ox3, CN 2-12 grossly intact. Moves all extremities spontaneously, 5/5 all extremities but had some fatigue and dropped to 4/5 with resistance. Cerebeller Neg
T: 36.4°C BP: 139/69 HR: 68 RR: 18 SpO2: 100% on room air
Gen: Awake, alert
HENT: Left ptosis
Neuro: A&Ox3, CN 2-12 grossly intact. Moves all extremities spontaneously, 5/5 all extremities but had some fatigue and dropped to 4/5 with resistance. Cerebeller Neg

1/ Instilling trust in the COVID-19 vaccine 💉- how do we address myths and legitimate concerns? Let’s take a moment to address some of them 👇🏼
2/ Here are some common myths and concerns:
1) Vaccines are not safe because of the quick roll-out/emergency use authorization
2) Vaccines are not safe for pregnant or breastfeeding women
3) Vaccines and clotting risks
What other myths/concerns have you heard?
1) Vaccines are not safe because of the quick roll-out/emergency use authorization
2) Vaccines are not safe for pregnant or breastfeeding women
3) Vaccines and clotting risks
What other myths/concerns have you heard?
3/ Watch the following helpful video addressing many of these issues:
1/ Let’s review pediatric sedation with Dr. Amy Alayari (PGY3)!
Classify the following level of sedation: someone is in a controlled state of depressed consciousness during which airway is maintained. Patient can respond to questions and light touch (e.g. “open your eyes”)
Classify the following level of sedation: someone is in a controlled state of depressed consciousness during which airway is maintained. Patient can respond to questions and light touch (e.g. “open your eyes”)
2/ Think of sedation as a continuum, understand that a patient can go from mild to general anesthesia within seconds! Review the slide here for the answer to the question above

3/ Always be prepared before giving sedation! That includes giving informed consent and making sure you have all materials in the SOAP-ME mnemonic ready

1/#Morningreport @SinaiBmoreIMRes
by @NasirAlhamdan featured a presentation of progressive fatigue and tachypnea X 2 months. This presentation opens up a significant number of #DDx's !
#MedTwitter #MedStudentTwitter
by @NasirAlhamdan featured a presentation of progressive fatigue and tachypnea X 2 months. This presentation opens up a significant number of #DDx's !
#MedTwitter #MedStudentTwitter

2/Other findings were:
-unexplained weight loss.,
- Tachypnea & mild SOB
- Intermittent chronic diarrhea, Intermittent small amount of bright blood per rectum
- Bruises on thighs
Now the DDx shift from the respiratory system to maybe an overlap of a hematologic etiology
-unexplained weight loss.,
- Tachypnea & mild SOB
- Intermittent chronic diarrhea, Intermittent small amount of bright blood per rectum
- Bruises on thighs
Now the DDx shift from the respiratory system to maybe an overlap of a hematologic etiology
3/A quick overview of our thoughts were:

1/#Morningreport @SinaiBmoreIMRes
featured a young patient presenting with abdominal pain X 2 weeks with a serum K=2.8.
There was also increased urinary frequency
some weakness and fatigue during the past 2 weeks
#DDX #MedTwitter #medstudents #FOAMed
featured a young patient presenting with abdominal pain X 2 weeks with a serum K=2.8.
There was also increased urinary frequency
some weakness and fatigue during the past 2 weeks
#DDX #MedTwitter #medstudents #FOAMed
2/The DDX for Hypokalemia requires consideration of a 3 pronged approach: 1)Decreased intake 2)Renal and GI losses and 3) IC shifts.

3/For the workup: Spot urine potassium and 24 hour urinary Potassium suggested urinary K wasting.
[UK] high (>40 mEq/L) =renal K loss
TTKG of 9 was concerning for renal potassium wasting
In hypokalemia (K⁺ <3.5 mEq/L), the TTKG > 7 suggests renal K wasting.
[UK] high (>40 mEq/L) =renal K loss
TTKG of 9 was concerning for renal potassium wasting
In hypokalemia (K⁺ <3.5 mEq/L), the TTKG > 7 suggests renal K wasting.


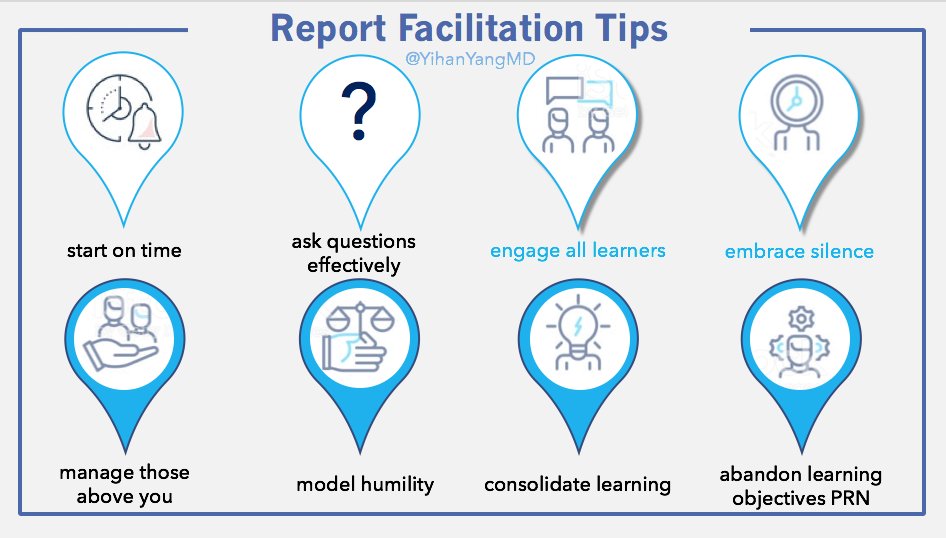
1/ #MedEdMethodsMonday #MorningReport edition ends this week with:
Tip 7-Abandon Objectives PRN
Tip 8-Consolidate Learning
#MedEd #MedTwitter #MedStudentTwitter #FacDev #MedEdPearls #ChiefResidents
Tip 7-Abandon Objectives PRN
Tip 8-Consolidate Learning
#MedEd #MedTwitter #MedStudentTwitter #FacDev #MedEdPearls #ChiefResidents

2/ Tip 7 - Abandon Objectives
The chief resident has started on time, asked questions, engaged learners, embraced silence, managed faculty, modeled humility...
Then says:
“Okay. We have 5 minutes left. Let’s quickly talk about this slide...”
😱🤯
The chief resident has started on time, asked questions, engaged learners, embraced silence, managed faculty, modeled humility...
Then says:
“Okay. We have 5 minutes left. Let’s quickly talk about this slide...”
😱🤯
3/ Abandon Objectives - Ever fill a water balloon?
Ever try to get the water balloon super juicy by trying to squeeze in that last drop of water and then have the whole thing sadly explode?
Teaching is like that.
Try to cram in too much knowledge and you risk losing it all.
Ever try to get the water balloon super juicy by trying to squeeze in that last drop of water and then have the whole thing sadly explode?
Teaching is like that.
Try to cram in too much knowledge and you risk losing it all.
1/ #MedEdMethodsMonday #MorningReport edition this wk:
Tips 5&6: Manage Faculty & Model Humility
See last 3 wks for: Start on ⏰ | Ask ? Effectively | Engage All Learners & Embrace Silence
#MedEd #ChiefResidents #MedEdPearls #FacDev #MedStudentTwitter #MedTweetorial
Tips 5&6: Manage Faculty & Model Humility
See last 3 wks for: Start on ⏰ | Ask ? Effectively | Engage All Learners & Embrace Silence
#MedEd #ChiefResidents #MedEdPearls #FacDev #MedStudentTwitter #MedTweetorial

2/ Tip5 Manage Faculty | The Opinions
Seems like faculty attendance @ morning report is all over the map.
Interestingly, when @StephenHolt7 and I conducted our multi-institute stakeholder interviews, many more residents said faculty SHOULDN’T be @ report than #Medtwitter did
Seems like faculty attendance @ morning report is all over the map.
Interestingly, when @StephenHolt7 and I conducted our multi-institute stakeholder interviews, many more residents said faculty SHOULDN’T be @ report than #Medtwitter did

3/ Manage Faculty | Conflicted
In fact, the tension between why faculty should be present @ report & why faculty shouldn’t be present was often palpable within the SAME interview.
Why?
In fact, the tension between why faculty should be present @ report & why faculty shouldn’t be present was often palpable within the SAME interview.
Why?
1/ #MedEdMethodsMonday, wk 3 of #MorningReport theme!
Now that you've 1) Started on time & 2)Asked ?s effectively...
Tip 3 Engage All Learners & Tip 4 Embrace Silence
#ChiefTips #MedEd #MedTwitter #MedStudentTwitter #MedEdPearls #FacDev
Now that you've 1) Started on time & 2)Asked ?s effectively...
Tip 3 Engage All Learners & Tip 4 Embrace Silence
#ChiefTips #MedEd #MedTwitter #MedStudentTwitter #MedEdPearls #FacDev
2/ Engage Learners - There are too many strategies to help engage all learners to cover them all. For this thread, I'll focus on:
⚡️Names
⚡️Microgroups
⚡️Deflection
⚡️Names
⚡️Microgroups
⚡️Deflection
3/ Engage Learners - Names
Use them!
Seems basic. How many reports have you been to where the facilitator did not use (or perhaps did not know) learners' names?
When I was a medical student, esp with a non-Western name, I can tell you it was near 100%
Use them!
Seems basic. How many reports have you been to where the facilitator did not use (or perhaps did not know) learners' names?
When I was a medical student, esp with a non-Western name, I can tell you it was near 100%
1/ Today’s #MedEdMethodsMonday continues the #MorningReport theme. Last week covered strategies for starting on time.
Today’s Tip 2 - Asking Questions Effectively!
#MedEd #MedEdPearls #Medtwitter #Medtweetorial #FacDev #MedStudentTwitter #ChiefResidents
Today’s Tip 2 - Asking Questions Effectively!
#MedEd #MedEdPearls #Medtwitter #Medtweetorial #FacDev #MedStudentTwitter #ChiefResidents
2/ Over the weekend, around 3/4 of respondents to the poll below said they sometimes felt uncomfortable asking learners directed questions while facilitating report:
3/ Cause of discomfort was a tie between not wanting to appear like “pimping,” and avoiding calling learners out.

1/ When trying to describe a rash to a derm consultant, do you ever plan to say maculopapular & just hope it's right? Fear no more, one of our wonderful residents, Lowell, shared this plain English approach to rashes in #morningreport
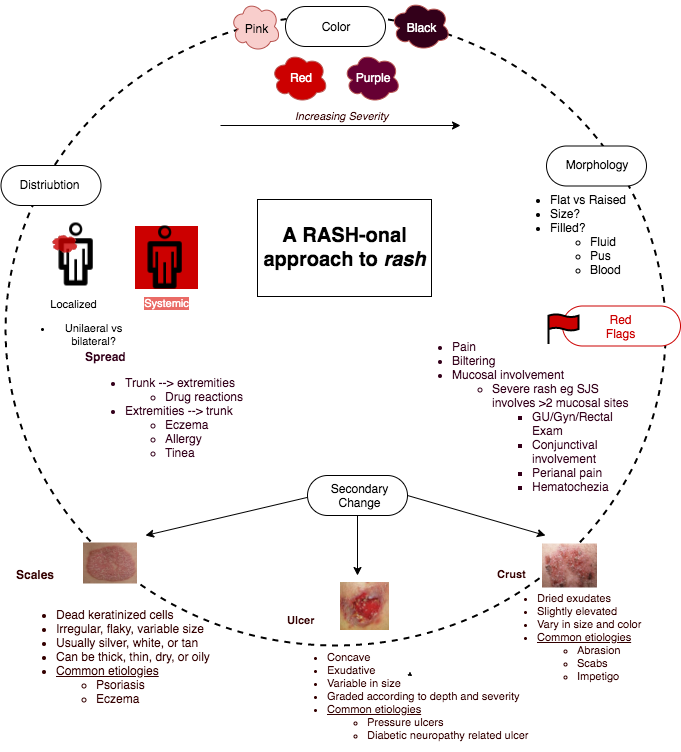
2/ Going clockwise around the circle, we had a case of a purple, mm sized, raised rash associated with pain and without secondary changes, and localized to the extremities, as seen here: slideshare.net/janinemagalhae…
3/ It’s our old friend, palpable purpura! In general, purpuric rash has an important differential diagnosis to consider, which is summarized in this flowsheet from Access Medicine, Clinical Dermatology:


Today I'm going to do a #Tweetorial on non-resolving pneumonia (NRP)! These are a series of pearls on a prior #MorningReport case that I gave earlier this year. We are going to cover definitions, differential diagnosis/schema & workup of NRP #IDTwitter #PulmTwitter
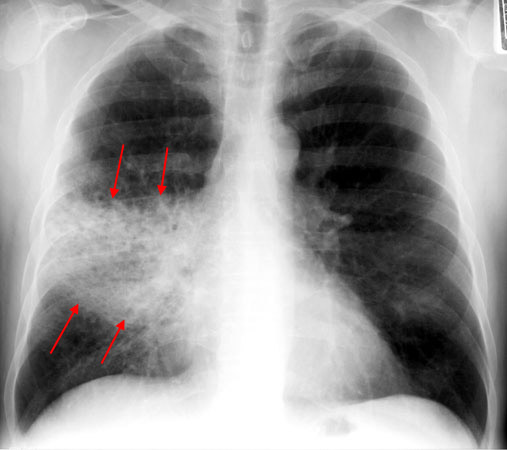
So first off, what is non-resolving pneumonia (NRP)?
It is a bit vague, but it's a lack of resolution of symptoms or radiographic findings over an expected time period despite appropriate antibiotic treatment.
It is a bit vague, but it's a lack of resolution of symptoms or radiographic findings over an expected time period despite appropriate antibiotic treatment.
Let's separate this term from "recurrent PNA", which consists of multiple episodes with symptom free intervals & radiologic clearance (e.g. aspiration PNA).
We will avoid the topic of "what is a pneumonia anyway?"
We will avoid the topic of "what is a pneumonia anyway?"
