Discover and read the best of Twitter Threads about #SpacedLearning
Most recents (10)

We didn't have a #Neuro case today on @CPSolvers #VMR with @AaronLBerkowitz but don't worry! Let's recap a prior episode for some #SpacedLearning @DxRxEdu @rabihmgeha
With @ddeng_22 @KannuBansalMD
clinicalproblemsolving.com/morning-report…
With @ddeng_22 @KannuBansalMD
clinicalproblemsolving.com/morning-report…
A 26 yo M w/ a PMH of nodular sclerosing hodgkins lymphoma p/w left-sided facial droop, L arm weakness, and dysarthria.
He presented 12 hours after onset and his symptoms had resolved.
3 months prior he had an autologous stem cell transplant and is currently on Brentuximab.
He presented 12 hours after onset and his symptoms had resolved.
3 months prior he had an autologous stem cell transplant and is currently on Brentuximab.
First of remembering that E=MC2
Time of onset and localization
Sudden Onset: Think stroke, seizure, Todd's paralysis, toxic metabolic, migraine with aura
Localization: Brainstem ipsilateral face and contralateral body
Time of onset and localization
Sudden Onset: Think stroke, seizure, Todd's paralysis, toxic metabolic, migraine with aura
Localization: Brainstem ipsilateral face and contralateral body

29M w severe persistent asthma p/w recurrent exacerbations despite optimal LABA/intranasal steroids. Abs eos 1250, total Ig E 1500, CT +mucus plugging, central bronchiectasis upper-middle lobes. Originally from Mexico, now in Texas. Which of the ff tests is indicated?
1/10
Great job! The majority got the right answer, allergic bronchopulmonary aspergillosis (ABPA).
Recurrent asthma exacerbations despite optimal asthma therapy & eosinophilia a/w mucus plugging and multilobar central bronchiectasis should raise suspicion for ABPA.
Great job! The majority got the right answer, allergic bronchopulmonary aspergillosis (ABPA).
Recurrent asthma exacerbations despite optimal asthma therapy & eosinophilia a/w mucus plugging and multilobar central bronchiectasis should raise suspicion for ABPA.
2/10
Aspergillosis, classified as saprophytic (aspergilloma), allergic (ABPA, hypersensitivity pneumonitis, allergic sinusitis), or invasive (pulmonary, other organs).
ABPA: hypersensitivity to A. fumigatus; can also occur from other fungi (referred as ABPM, M for mycosis).
Aspergillosis, classified as saprophytic (aspergilloma), allergic (ABPA, hypersensitivity pneumonitis, allergic sinusitis), or invasive (pulmonary, other organs).
ABPA: hypersensitivity to A. fumigatus; can also occur from other fungi (referred as ABPM, M for mycosis).

1/
OMG! I had an awesome #MedEd breakthrough this week.
SOOOO PUMPED!
And guess what? Consider this #spacedlearning because it all loops back to my Monday meeting with one of my #mentors @dan_p_hunt_MD.
Wanna hear about it? You do? Good! 😁
OMG! I had an awesome #MedEd breakthrough this week.
SOOOO PUMPED!
And guess what? Consider this #spacedlearning because it all loops back to my Monday meeting with one of my #mentors @dan_p_hunt_MD.
Wanna hear about it? You do? Good! 😁

2/
Okay, so one of the agenda items was about my struggles with clinical teaching during #COVID19.
Specifically:
When I can’t bedside round or have the students or whole team go in due to a patient being a #PUI or #COVID19+, it’s limiting my teachable moments.
Waaah.😢
Okay, so one of the agenda items was about my struggles with clinical teaching during #COVID19.
Specifically:
When I can’t bedside round or have the students or whole team go in due to a patient being a #PUI or #COVID19+, it’s limiting my teachable moments.
Waaah.😢
3/
Dan suggested I try this:
1. Bring my mini-whiteboard
2. Assign a question to the students while I go into isolation room with resident or intern.
3. Leave them with the board/marker and allow them to rapid fire search on whatever devices or computers.
Cool right?
Dan suggested I try this:
1. Bring my mini-whiteboard
2. Assign a question to the students while I go into isolation room with resident or intern.
3. Leave them with the board/marker and allow them to rapid fire search on whatever devices or computers.
Cool right?
Part 1/2 📌
32/M w/ 6 wks fever, abd pain, weight loss. Exam: tender RUQ, hepatomegaly. 🧪: WBC 3.1, Hgb 8, Plt 110; AST 62, ALT 70, Alk Phos 450, bili 0.8; RPR(-). HIV came back +, CD4 89. CT: scattered tiny heterogenous liver lesions. Path shown👇[Go to next tweet]
32/M w/ 6 wks fever, abd pain, weight loss. Exam: tender RUQ, hepatomegaly. 🧪: WBC 3.1, Hgb 8, Plt 110; AST 62, ALT 70, Alk Phos 450, bili 0.8; RPR(-). HIV came back +, CD4 89. CT: scattered tiny heterogenous liver lesions. Path shown👇[Go to next tweet]


Part 2/2 📌 [case continued]
Path shown👆: multiple dilated blood-filled spaces surrounded by clumps of Warthin-Starry+ rods, AFB stain (-). Lives in Florida, no travel, previously healthy, worked as a cashier, no pets. What is the most likely opportunistic infection?
Path shown👆: multiple dilated blood-filled spaces surrounded by clumps of Warthin-Starry+ rods, AFB stain (-). Lives in Florida, no travel, previously healthy, worked as a cashier, no pets. What is the most likely opportunistic infection?
1/12
The majority got this one right - Bartonella. As @k_vaishnani @JosGilbertoMon1 @NateWarnerMD @Elennaro @ArmelleID correctly pointed, this is indeed a case of ⚡️bacillary peliosis (BP).
@MedTweetorials
Pictures taken from: bit.ly/3joTS2m
The majority got this one right - Bartonella. As @k_vaishnani @JosGilbertoMon1 @NateWarnerMD @Elennaro @ArmelleID correctly pointed, this is indeed a case of ⚡️bacillary peliosis (BP).
@MedTweetorials
Pictures taken from: bit.ly/3joTS2m
28/F fom Bolivia, no PMH, referred to you for a +Trypanosoma cruzi serology. No SSx, has normal EKG (w/ 30 sec strip), CXR & echo. Which of the following complications of Chagas’ disease has the most evidence to support treating her with benznidazole to reduce risk?
1/14
Only 1/3 got the correct answer: vertical transmission.
Although most patients with indeterminate Chagas are treated w/ benznidazole, there is limited data on the effect of Rx to progression to cardiomyopathy/GI involvement (partly because it requires decades of ffup).
Only 1/3 got the correct answer: vertical transmission.
Although most patients with indeterminate Chagas are treated w/ benznidazole, there is limited data on the effect of Rx to progression to cardiomyopathy/GI involvement (partly because it requires decades of ffup).
2/14
There is also limited data (& no broad consensus) in treating indeterminate Chagas in patients who are at risk for reactivation (e.g. HIV, those undergoing transplant). bit.ly/2z3p5Fs bit.ly/2z00jpM
There is also limited data (& no broad consensus) in treating indeterminate Chagas in patients who are at risk for reactivation (e.g. HIV, those undergoing transplant). bit.ly/2z3p5Fs bit.ly/2z00jpM
#idgrandrounds
1/2
68/M +progressive L facial/arm numbness & weakness, R hip pain x 6 wks. +malaise/wt loss but no fever. Exam: no rashes, +dysarthria. Labs: U/R.
Brain MRI: 2x2 cm R thalamic mass w/ vaso edema
CT: speculated RUL mass, sclerotic R iliac crest/SI joint
👇
1/2
68/M +progressive L facial/arm numbness & weakness, R hip pain x 6 wks. +malaise/wt loss but no fever. Exam: no rashes, +dysarthria. Labs: U/R.
Brain MRI: 2x2 cm R thalamic mass w/ vaso edema
CT: speculated RUL mass, sclerotic R iliac crest/SI joint
👇
2/2
Lives in rural IL near a creek. Stays at home w/ a dog. Loves to garden. No travel, incarceration.
Neurosurgery performed burr hole/biopsy of mass (c/f glioblastoma). ID was consulted when biopsy came out.
What is your ddx/dx? @TxID_Edu @jdcooperid @GermHunterMD
Lives in rural IL near a creek. Stays at home w/ a dog. Loves to garden. No travel, incarceration.
Neurosurgery performed burr hole/biopsy of mass (c/f glioblastoma). ID was consulted when biopsy came out.
What is your ddx/dx? @TxID_Edu @jdcooperid @GermHunterMD
1/11 Biopsy of brain mass: broad-based budding yeast, Cx: Blastomyces dermatitidis. Urine Histo Ag: low positive
CASE RESOLUTION: Disseminated blastomycosis
@LemuelNonMD @TxID_Edu @Cortes_Penfield @KartikAcharyaID @IDdoc_Vetri @jdcooperid got the correct Dx/Ddx! Thank you.
CASE RESOLUTION: Disseminated blastomycosis
@LemuelNonMD @TxID_Edu @Cortes_Penfield @KartikAcharyaID @IDdoc_Vetri @jdcooperid got the correct Dx/Ddx! Thank you.

Teaching Rounds Day 3
Anemia - Part 1
Neighbors and Time Zones...
Join us #medtwitter & #medstudenttwitter
Anemia - Part 1
Neighbors and Time Zones...
Join us #medtwitter & #medstudenttwitter
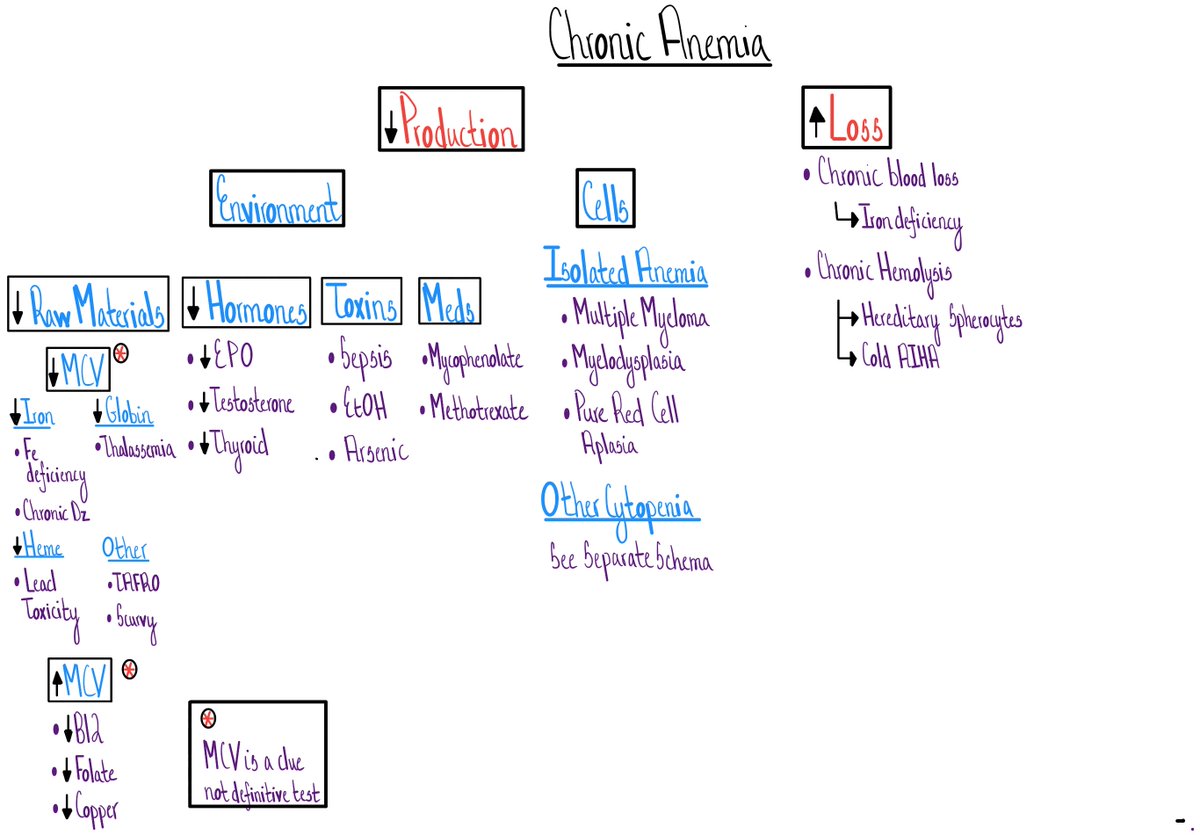
Claim:
It's nearly impossible to have an approach to anemia.
Yup, impossible.
It's as tough as having an approach to altered mental status?
Wait, what?
Wasn't that the VERY first @cpsovlers episode?
And...what about this schema??
It's nearly impossible to have an approach to anemia.
Yup, impossible.
It's as tough as having an approach to altered mental status?
Wait, what?
Wasn't that the VERY first @cpsovlers episode?
And...what about this schema??

Well, we lied.
Sort of.
That's an approach to ACUTE altered mental status.
Not just any old altered mental status....
Sort of.
That's an approach to ACUTE altered mental status.
Not just any old altered mental status....
21/M w/ 2 days abrupt fever, sore throat. No cough/rhinorrhea, rigors, hoarseness. Exam: b/l tonsil exudates, +tender cervical LAD, no neck swelling. No PMH, allergies. Sexually active w/ female partners, no prior STI. 4th gen HIV(-), rapid Strep(-). W/c of the ff is correct?
1/16
Strictly based on guidelines, 31% got the correct answer -- observe/counsel. At some point in our practice, we might have done any of the above choices, which might seem reasonable.
The goal of the Tweetorial is to discuss evidence behind Abx prescription for pharyngitis.
Strictly based on guidelines, 31% got the correct answer -- observe/counsel. At some point in our practice, we might have done any of the above choices, which might seem reasonable.
The goal of the Tweetorial is to discuss evidence behind Abx prescription for pharyngitis.
2/16
Respiratory viruses cause the majority of acute pharyngitis (up to 45%). Group A Strep (GAS) is the major bacterial cause & the main indication for Abx. But, it comprises only 10% of acute pharyngitis (higher in other areas).
Respiratory viruses cause the majority of acute pharyngitis (up to 45%). Group A Strep (GAS) is the major bacterial cause & the main indication for Abx. But, it comprises only 10% of acute pharyngitis (higher in other areas).
February Teaching Rounds - Recap
Part 1 of 2.
Because #spacedlearning is an endless journey...
Join us #medtwitter & #medstudenttwitter
Part 1 of 2.
Because #spacedlearning is an endless journey...
Join us #medtwitter & #medstudenttwitter
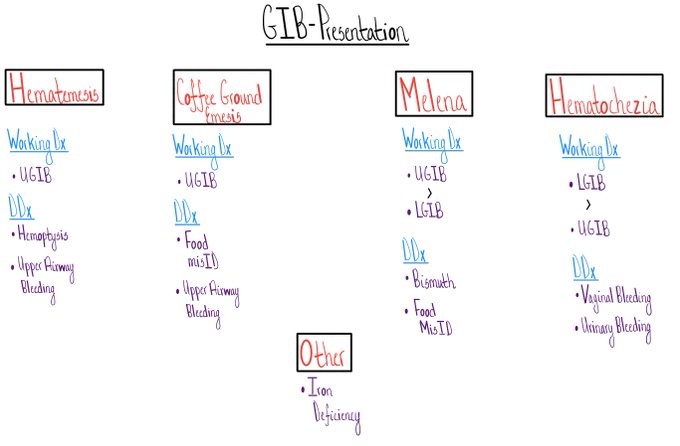
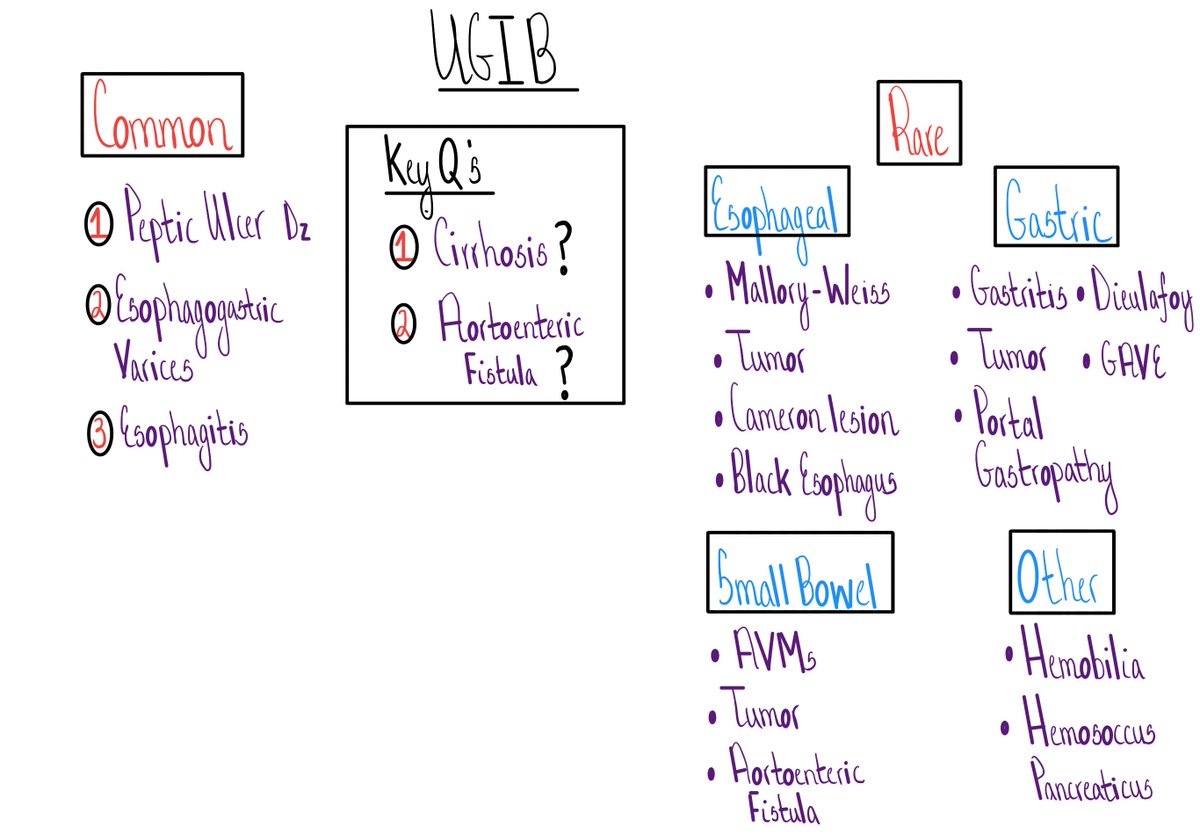
Day 2 - Upper GI bleed
1. 4 common pathways to a working Dx of an overt upper GI bleed
2. 3 common diagnosis...
3. 2 KEY questions!
More here -
bit.ly/2V9pboc
1. 4 common pathways to a working Dx of an overt upper GI bleed
2. 3 common diagnosis...
3. 2 KEY questions!
More here -
bit.ly/2V9pboc
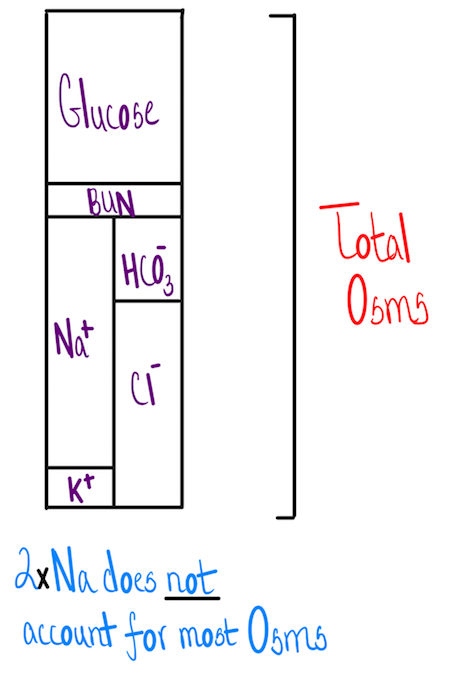
Day 3 - H20 toxicity
1. Hyponatremia = excess H20 = H20 toxicity.
The is true is most, but not all cases
2. Why do we care?
When neurons swell they don't work well...
3. @jackpenner's @CPSolvers video & schema bit.ly/3b64K0T
More here - bit.ly/3bUWUri
1. Hyponatremia = excess H20 = H20 toxicity.
The is true is most, but not all cases
2. Why do we care?
When neurons swell they don't work well...
3. @jackpenner's @CPSolvers video & schema bit.ly/3b64K0T
More here - bit.ly/3bUWUri
#idgrandrounds
48F, bitten by a monkey at a zoo. She calls her primary who then calls you for advice.
What Qs should you ask? What infections should you be worried about? @TxID_Edu @Cortes_Penfield @BradCutrellMD @jdcooperid
Have you had a consult on monkey bite before?
48F, bitten by a monkey at a zoo. She calls her primary who then calls you for advice.
What Qs should you ask? What infections should you be worried about? @TxID_Edu @Cortes_Penfield @BradCutrellMD @jdcooperid
Have you had a consult on monkey bite before?
@TxID_Edu @Cortes_Penfield @BradCutrellMD @jdcooperid 1/15
Great! Thank you for ALL your responses. Speical thanks to @TxID_Edu @vivax74 @VarunPhadke2 @10minus6cosm for referencing additional resources.
Hope this tweetorial helps, especially those who may get consulted on monkey bite/exposure in the future.
Follow the thread 👇
Great! Thank you for ALL your responses. Speical thanks to @TxID_Edu @vivax74 @VarunPhadke2 @10minus6cosm for referencing additional resources.
Hope this tweetorial helps, especially those who may get consulted on monkey bite/exposure in the future.
Follow the thread 👇
2/15
𝐖𝐡𝐚𝐭 𝐢𝐧𝐟𝐞𝐜𝐭𝐢𝐨𝐧𝐬 𝐬𝐡𝐨𝐮𝐥𝐝 𝐲𝐨𝐮 𝐛𝐞 𝐰𝐨𝐫𝐫𝐢𝐞𝐝 𝐚𝐛𝐨𝐮𝐭?
A LOT, but the most important ones are:
1⃣ Herpes B
2⃣ Rabies
3⃣ Tetanus
Let's talk a little bit more about Herpes B and rabies 👇
𝐖𝐡𝐚𝐭 𝐢𝐧𝐟𝐞𝐜𝐭𝐢𝐨𝐧𝐬 𝐬𝐡𝐨𝐮𝐥𝐝 𝐲𝐨𝐮 𝐛𝐞 𝐰𝐨𝐫𝐫𝐢𝐞𝐝 𝐚𝐛𝐨𝐮𝐭?
A LOT, but the most important ones are:
1⃣ Herpes B
2⃣ Rabies
3⃣ Tetanus
Let's talk a little bit more about Herpes B and rabies 👇
