Discover and read the best of Twitter Threads about #AntibioticStewardship
Most recents (4)

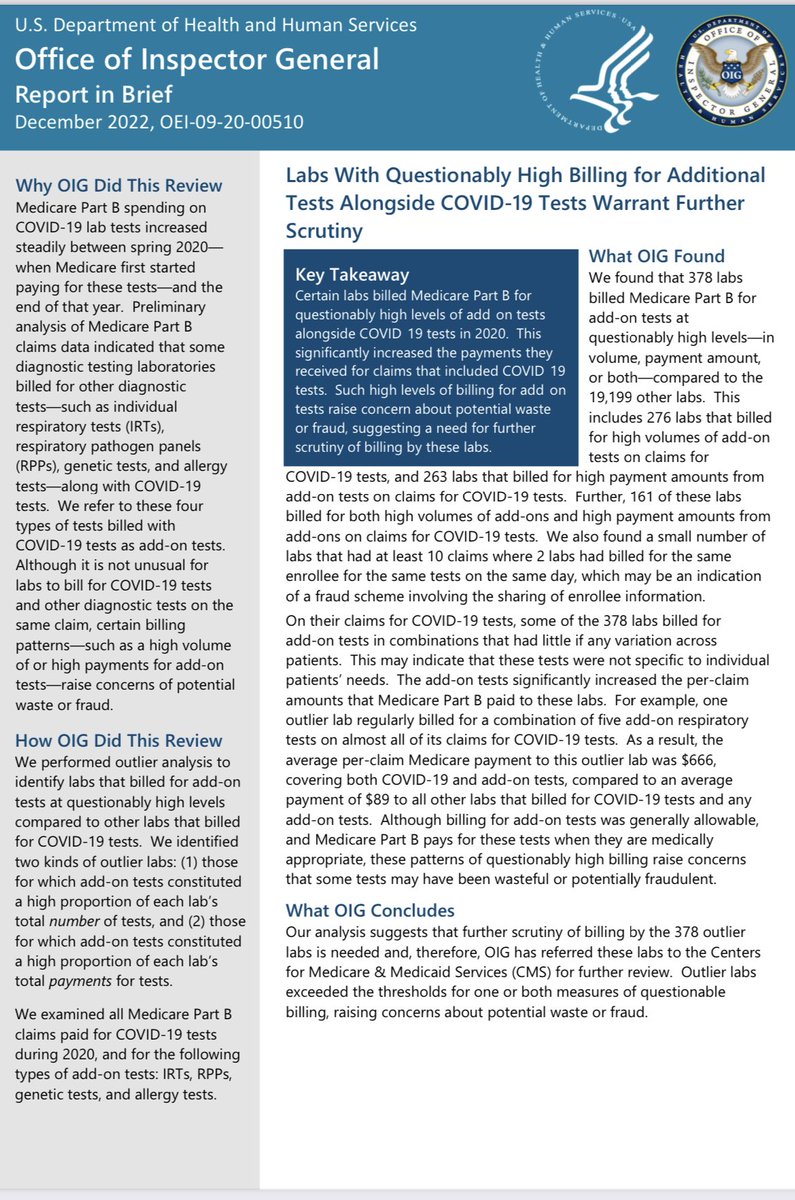
CDC: You must rule out other viruses including #influenza #RSV during pandemic when testing #COVID19 OIG: if you do that, U should be investigated for fraud and abuse. 😵💫😵💫😵💫 @BioFireDX & @QIAGEN are the best #covidtests for patients who feel sick. FULL STOP. Despite JDs advice 



cdc.gov/flu/profession… GEEZ WHY CAN’T WE FIND COVID TESTING ANYWHERE??? Despite best medical practice, OIG wants to investigate you for doing what’s right for the patient, then the lawyers will decide. Who will offer tests with that Damocletian risk.
To be clear there is zero need to do allergy skin testing OR PGX pharmacogenomic tests when evaluating for COVID testing. Lumping the first FDA approved #COVID19 test with these shows how bad lawyers are at understanding medical care. Yet all too willing to attack good docs/labs



Antibiotikaresitenzen sind eine gesundheitspolitische Herausforderung, die uns noch Jahrzehnte begleiten wird.
Wir brauchen endlich flächendeckende Schulungen zum differenzierten und rationalen Antibiotika-Einsatz unter Ärzten und sonstigem Fachpersonal.
#AntibioticStewardship
Wir brauchen endlich flächendeckende Schulungen zum differenzierten und rationalen Antibiotika-Einsatz unter Ärzten und sonstigem Fachpersonal.
#AntibioticStewardship
Die @ECDC_EU schätzt, dass jährlich rund 35000 Todesfälle die folge von Antibiotika-Resistenzen sind, die Tendenz ist trotz Rückgängen im Antibiotika-Verbrauch abgesehen vom Pandemie-Jahr 2020 bei allen Infektionen und Erregern steigend.
tagesschau.de/inland/antibio…
tagesschau.de/inland/antibio…
Gravierend finde ich immer noch den Ländervergleich, welcher klar zeigt, dass es sich auszahlt, hier Geld und Personal zu investieren.
Egal ob Infektionen, Todesfällen oder DALYs, es ziehen sich deutliche Grenzen durch Europa. Deutschland ist hier bestenfalls Mittelfeld.
Egal ob Infektionen, Todesfällen oder DALYs, es ziehen sich deutliche Grenzen durch Europa. Deutschland ist hier bestenfalls Mittelfeld.


I studied >200 pages on Clinical Documentation Improvement.
(So you don’t have to)
Here are 3 documenting tips so you (and your hospital) get paid.
(Repost with actual 🧵 this time)
(So you don’t have to)
Here are 3 documenting tips so you (and your hospital) get paid.
(Repost with actual 🧵 this time)
The problem?
• Hospitals are PAID off documentation (even surgeries)
• Documentation needs to be specific & accurate
• Doctors language ≠ coding language
Let’s dig in…
• Hospitals are PAID off documentation (even surgeries)
• Documentation needs to be specific & accurate
• Doctors language ≠ coding language
Let’s dig in…
1. You CAN code off of probability.
You’re a doctor. You can make a clinical diagnosis. You do not need perfect objective data to prove it.
“Presumed” or “suspected” is okay.
(For inpatient only. Sorry outpatient docs)
An example…
You’re a doctor. You can make a clinical diagnosis. You do not need perfect objective data to prove it.
“Presumed” or “suspected” is okay.
(For inpatient only. Sorry outpatient docs)
An example…

High yield talk by Pablo Sanchez at #IDWeek2020 session Antimicrobial Stewardship in Pediatric ICUs excellent bundle for #NICU #antibioticstewardship @eerogersmd @PfaffMd excellent work highlighted by @InfectiousNeo @PedsPharmD

Great summary of the harms of broad spectrum antibiotics in #NICU - greeter risk with cephalosporin > aminoglycoside-based therapy
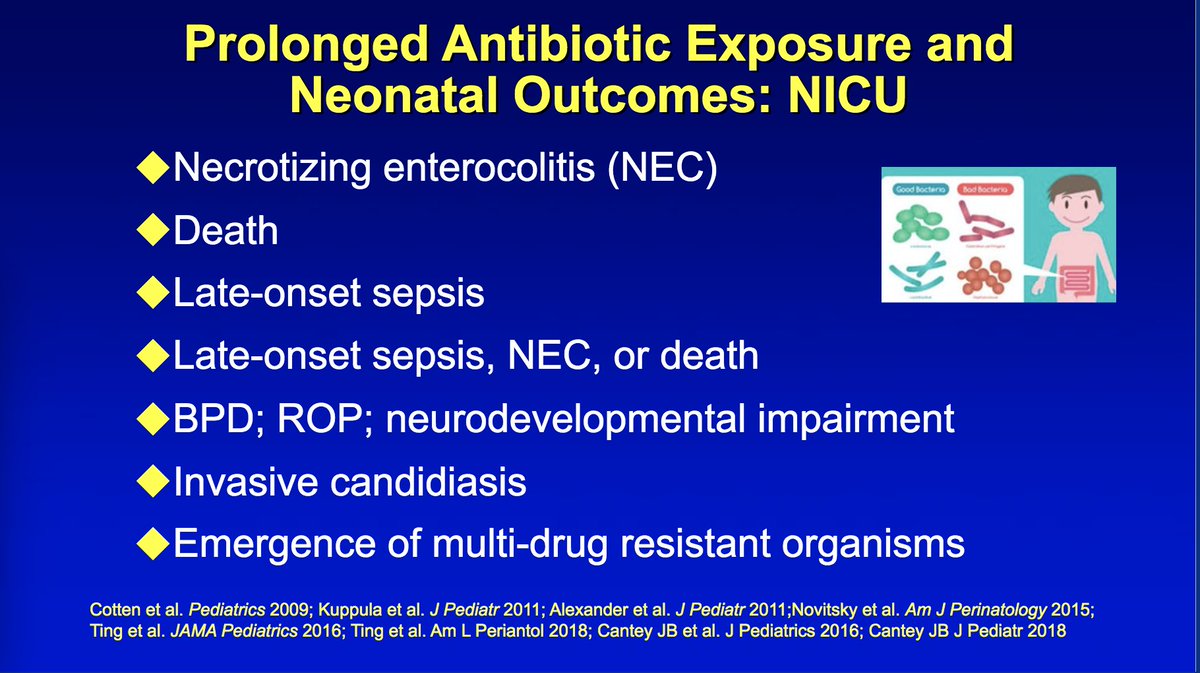
Each additional day adds risk and combined with what we know from @PedsPharmD oral abstract on Global PPS there is a lot of variability in duration - big opportunity to standardize & shorten

