Discover and read the best of Twitter Threads about #ASCO23
Most recents (16)

@TumorBoardTues @JohnEbbenMDPhD #TumorBoardTuesday
📣Welcome as we summarize some of the incredible data from #ASCO23
👉There was SO much to take in, that even focusing on GI Cancers was a challenge
🙏As always, these were the🧑🏫that caught OUR interest, but this is not a judgement on those we do not highlight‼️
📣Welcome as we summarize some of the incredible data from #ASCO23
👉There was SO much to take in, that even focusing on GI Cancers was a challenge
🙏As always, these were the🧑🏫that caught OUR interest, but this is not a judgement on those we do not highlight‼️
@TumorBoardTues @JohnEbbenMDPhD 1/21
#TumorBoardTuesday
🤔Speaking for myself, @knutjla ‘s data has shaken my practice the most (including twice last week)
👉He presented the NORPACT-1 trial of peri-operative FOLFIRINOX vs. upfront🔪for resectable #PancreaticCancer
#TumorBoardTuesday
🤔Speaking for myself, @knutjla ‘s data has shaken my practice the most (including twice last week)
👉He presented the NORPACT-1 trial of peri-operative FOLFIRINOX vs. upfront🔪for resectable #PancreaticCancer

@TumorBoardTues @JohnEbbenMDPhD @knutjla @MDAkhilChawla @FlavioRochaMD @NbmerchantMD @MadameSurgeon @NirajGusani @TsengJennifer 2/21
#TumorBoardTuesday
✅@knutjla🗣️a well designed, well run trial
✅The authors even hypothesized a 20%⬆️in mOS
➡️However, pre-operative chemotherapy led to a significant⬇️in 18 month mOS😲
👉Despite a much better R0 resection rate
🤔What are your thoughts💭❓
#TumorBoardTuesday
✅@knutjla🗣️a well designed, well run trial
✅The authors even hypothesized a 20%⬆️in mOS
➡️However, pre-operative chemotherapy led to a significant⬇️in 18 month mOS😲
👉Despite a much better R0 resection rate
🤔What are your thoughts💭❓


Let's have a closer look 🧐at the PROSPECT trial after its presentation at #ASCO23 and publication in @NEJM bit.ly/43L83oI #radonc #crcsm 1/n
First of all, the study team is to be congratulated for successful recruitment and completion of the study. Almost 1200 patients randomized - everyone who has led a multicenter trial can appreciate how challenging it can be to keep recruitment up over time.
The study enrolled patients with locally advanced rectal cancer that had to meet some specific inclusion criteria.
🔹Tumor located 5-12 cm from anal verge
🔹Sphincter sparing surgery possible at baseline
🔹Distance from MRF min. 3 mm
🔹T2N1 or T3N- or T3 N1
Exclusion:
♦️T4
🔹Tumor located 5-12 cm from anal verge
🔹Sphincter sparing surgery possible at baseline
🔹Distance from MRF min. 3 mm
🔹T2N1 or T3N- or T3 N1
Exclusion:
♦️T4

1/ My time-to-tweet interval re: #ASCO23 myeloma abstracts is longer than my time-to-toci with CAR-T, but finally off 🏥 service and excited to tweet about a few #MMsm gems!
My research focuses on ⬇️ AEs, ⬇️ time tox, & improved workflows. Here are a few that stood out to me:
My research focuses on ⬇️ AEs, ⬇️ time tox, & improved workflows. Here are a few that stood out to me:
2/ @bhemato et al, CARTITUDE-4 (cilta-cel in #MMsm 1-3 prior lines).
Beyond dramatic PFS benefit, worth 🔨 home that CAR-T "one & done" (visits become ≤1x per month) vs DPd/VPd [even stronger DKd] always ≥1x visit/month.
Time tox advantage to CAR-T!
meetings.asco.org/abstracts-pres…
Beyond dramatic PFS benefit, worth 🔨 home that CAR-T "one & done" (visits become ≤1x per month) vs DPd/VPd [even stronger DKd] always ≥1x visit/month.
Time tox advantage to CAR-T!
meetings.asco.org/abstracts-pres…

3/ @adamssperling et al, PHE885 rapidly manufactured CAR-T with ⬇️ T-cell exhaustion.
Bridging before #MMsm CAR-T unlikely to ≥PR but likely to worsen cytopenias.
⬇️ vein-to-vein time to ~2 weeks: less bridging, happier bone marrow, happier patients!
meetings.asco.org/abstracts-pres…
Bridging before #MMsm CAR-T unlikely to ≥PR but likely to worsen cytopenias.
⬇️ vein-to-vein time to ~2 weeks: less bridging, happier bone marrow, happier patients!
meetings.asco.org/abstracts-pres…


Cilta-cel for early relapsed myeloma.
A deep dive-thread where we analyze this trial in incredible detail, all the nuances and subtleties.
Critical appraisal in patient/trainee friendly langauge.
Link to paper:
nejm.org/doi/full/10.10…
#mmsm
#ASCO23
A deep dive-thread where we analyze this trial in incredible detail, all the nuances and subtleties.
Critical appraisal in patient/trainee friendly langauge.
Link to paper:
nejm.org/doi/full/10.10…
#mmsm
#ASCO23
Trial was a comparison of cilta-cel to investigators choice of either dara/pom/dex (86.7% of patients received this) or velcade/pom/dex (12.3% of pts).
Authors write this control arm as "highly effective" standard of care therapy. Was it?
Authors write this control arm as "highly effective" standard of care therapy. Was it?

So unlike the ide-cel study (KARMMA-3), this trial enrolled patients that were not triple refractory (only 15%)- and only 21% of patients were refractory to daratumumab. Only 21% of patients refractory to carfilzomib.
Hence dara or isa + carfilzomib/dex should have been allowed
Hence dara or isa + carfilzomib/dex should have been allowed


Great review of proton CSI for pts w LMD: CNS PFS prolonged by 5mo. @JYangMDPhD This becomes SO pertinent as @LevineCancer @AtriumHealth prepares to open the 1st proton center in NC! #brainmets #btsm #asco23 1/



I have been asked several questions about the #ASCO23 abstract:
Durability of Responses With Biweekly Dosing of Teclistamab in Patients With Relapsed/Refractory Multiple Myeloma Achieving a Clinical Response in the MajesTEC-1 Study (8034), wanted to create a 🧵 for #mmsm… twitter.com/i/web/status/1…
Durability of Responses With Biweekly Dosing of Teclistamab in Patients With Relapsed/Refractory Multiple Myeloma Achieving a Clinical Response in the MajesTEC-1 Study (8034), wanted to create a 🧵 for #mmsm… twitter.com/i/web/status/1…
What were the criteria for switching to less frequent dosing schedules?
• In phase 1, patients had the option to switch from weekly to Q2W (every other week) dosing if they had achieved at least a partial response and at least 4 cycles of treatment
• In phase 2, patients had… twitter.com/i/web/status/1…
• In phase 1, patients had the option to switch from weekly to Q2W (every other week) dosing if they had achieved at least a partial response and at least 4 cycles of treatment
• In phase 2, patients had… twitter.com/i/web/status/1…
Given the rapid and deep responses, why did so many patients not switch (41/104 responders) to the less frequent dosing schedule?
• Switching was not mandated, but optional, for any patient who met the response criteria. This, in addition to the requirement for patients to… twitter.com/i/web/status/1…
• Switching was not mandated, but optional, for any patient who met the response criteria. This, in addition to the requirement for patients to… twitter.com/i/web/status/1…
Quick recap of outstanding talk by @adrienne_boire 👉🏻 we MUST open our minds to seek out LMD. Do the LPs, send the csf (esp CTCs), look for tx options/ trials. #btsm #asco23 1/


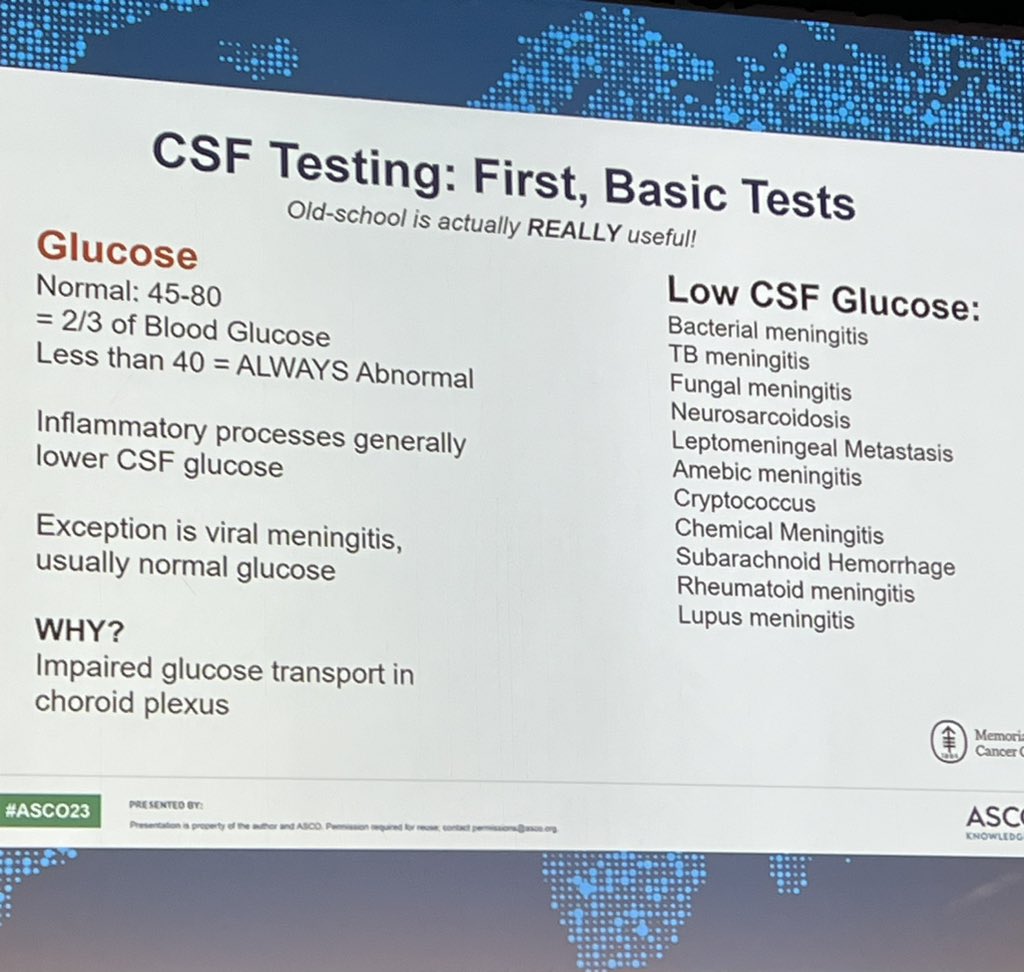
Imaging is 1st step. But "all that glitters isn"t gold." Esp consider this for pts on immunotx. Sens of MRI 71-100%. Slide 3 w broad ddx #asco23 2/



What csf studies? 3/




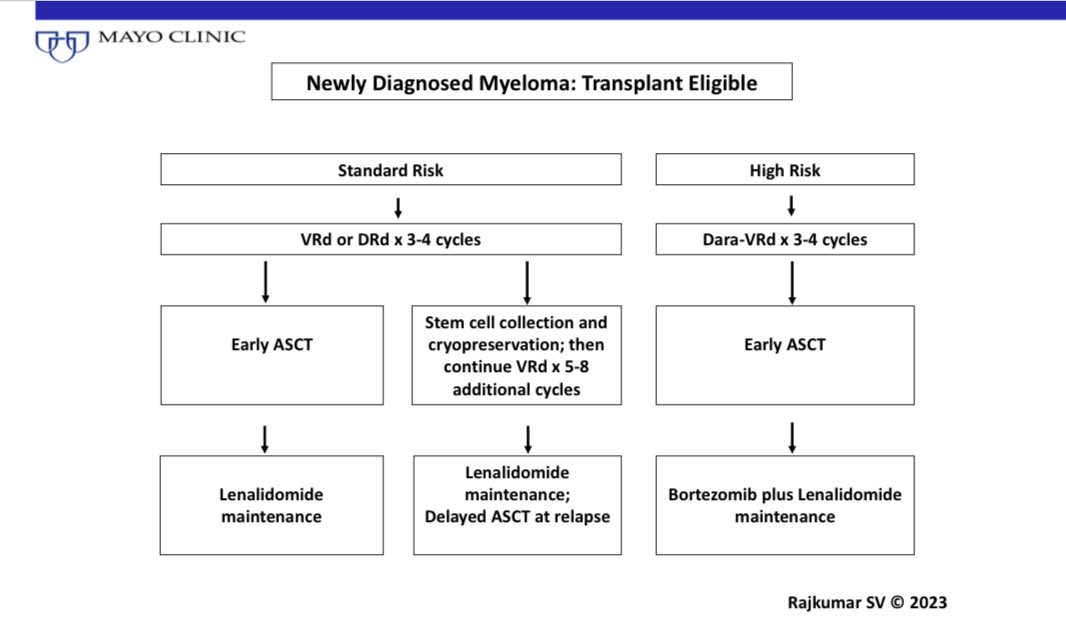
Newly diagnosed, not eligible for transplant.

First relapse

Today's announcement of data from #Indigo is a HUGE milestone for these pts & their families. #IDH #btsm 👉🏻 nejm.org/doi/full/10.10… 13/
Pts w grade 2 tumors & no tx aside from surgery, took placebo or po #vorasidenib. mPFS: 27.7 mo vs placebo 11.1 mo. Time to next intervention was longer in vorasidenib arm. (HR, 0.26; 95% CI, 0.15 to 0.43; P<0.001). 14/
In light of today's plenary @ASCO #asco23 👀
Grade 2 gliomas👉🏻 a tutorial. #btsm
Considered a low-grade glioma, but also considered to be a terminal illness. How? These tumors are incurable and affect adults, teens, & children. #asco23 1/
Grade 2 gliomas👉🏻 a tutorial. #btsm
Considered a low-grade glioma, but also considered to be a terminal illness. How? These tumors are incurable and affect adults, teens, & children. #asco23 1/
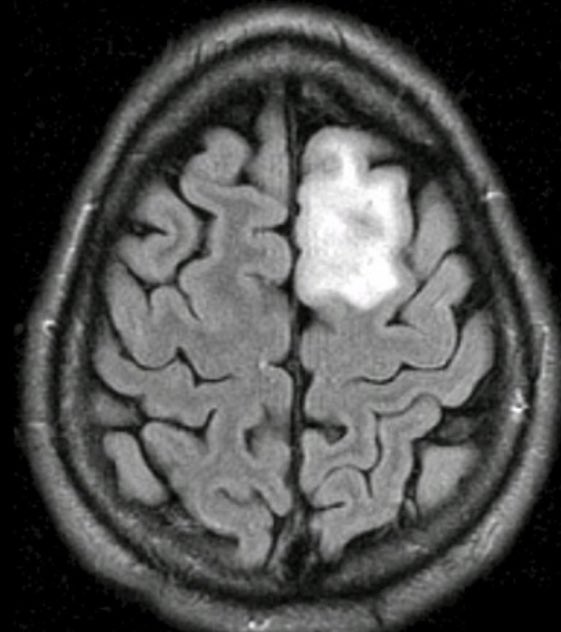
They are insidious and will sometimes stay quiet for years. They may be oligodendrogliomas (aka lazy tumors) or the more aggressive astrocytomas. I often tell my pts that grade 2 tumors have 2 goals in life: grow BIGGER and/ or change to a more aggressive form. 2/
On the imaging, they often do not enhance, and can sometimes be missed. The key is to look at T2 and flair images. These pts must be monitored closely because the tumors can become motivated to change at any time. 3/


#ASCO23 Tweetorial on putting results of PEACE-1 in context. Here we go!
@ASCO @ASTRO_org @HimanshuNagarMD @DrRanaMcKay @AlbertoBossial @Prof_Nick_James @PCaParker
@ASCO @ASTRO_org @HimanshuNagarMD @DrRanaMcKay @AlbertoBossial @Prof_Nick_James @PCaParker
1/n
ADT + tx intensification w/ chemo or ARSI is SOC based on lots of RCTs
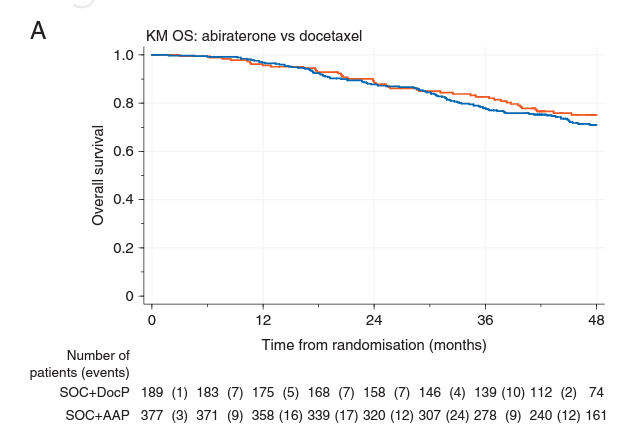
No OS diff seen in STAMPEDE from ADT+Abi vs ADT+doce (FFS difference as ARSI suppress PSA = FFS).
No clear role of triplet therapy in low volume (ARASENS)
Thus, SOC is ADT+doce or ARSI for low volume
ADT + tx intensification w/ chemo or ARSI is SOC based on lots of RCTs
No OS diff seen in STAMPEDE from ADT+Abi vs ADT+doce (FFS difference as ARSI suppress PSA = FFS).
No clear role of triplet therapy in low volume (ARASENS)
Thus, SOC is ADT+doce or ARSI for low volume

2/n
RT to primary for low volume improved FFS and OS in STAMPEDE arm H, and in IPD meta-analysis w/ HORRAD RCT.
18% of men received ADT+doce on STAMPEDE arm H, and no interaction of differential effect noticed.
Thus, ADT+doce+RT in low volume was the SOC at this point.
RT to primary for low volume improved FFS and OS in STAMPEDE arm H, and in IPD meta-analysis w/ HORRAD RCT.
18% of men received ADT+doce on STAMPEDE arm H, and no interaction of differential effect noticed.
Thus, ADT+doce+RT in low volume was the SOC at this point.

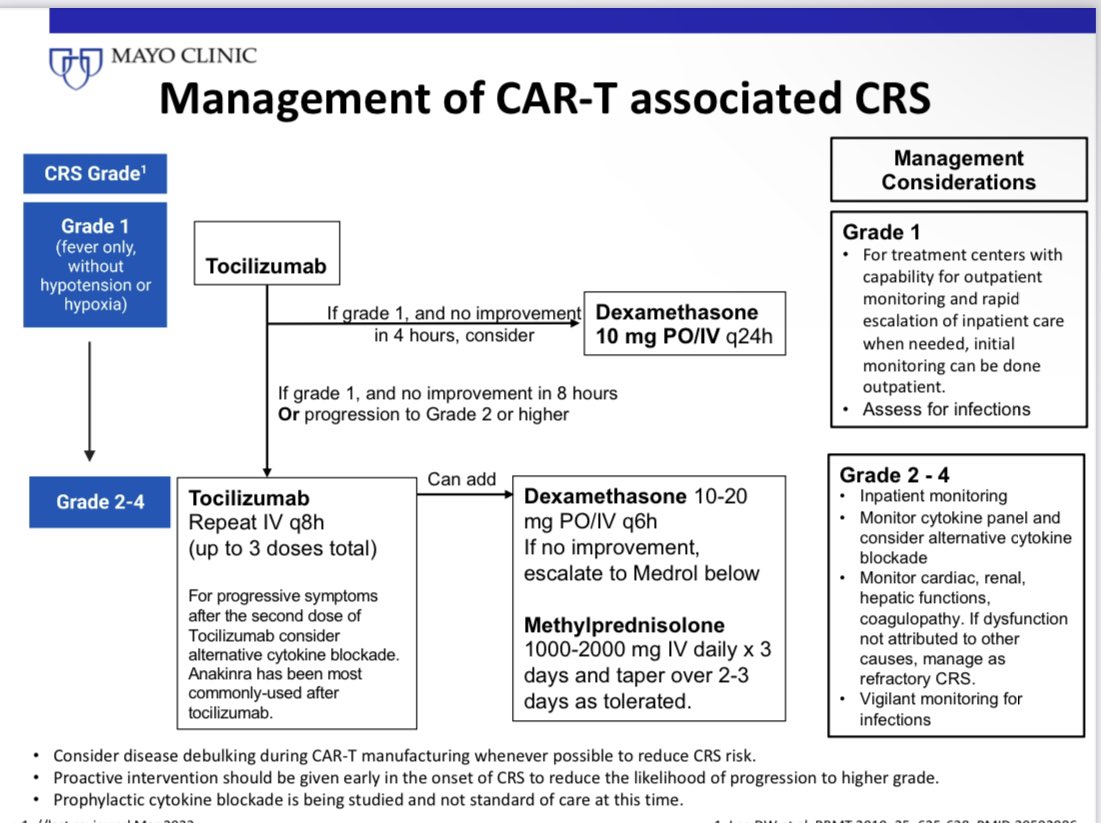
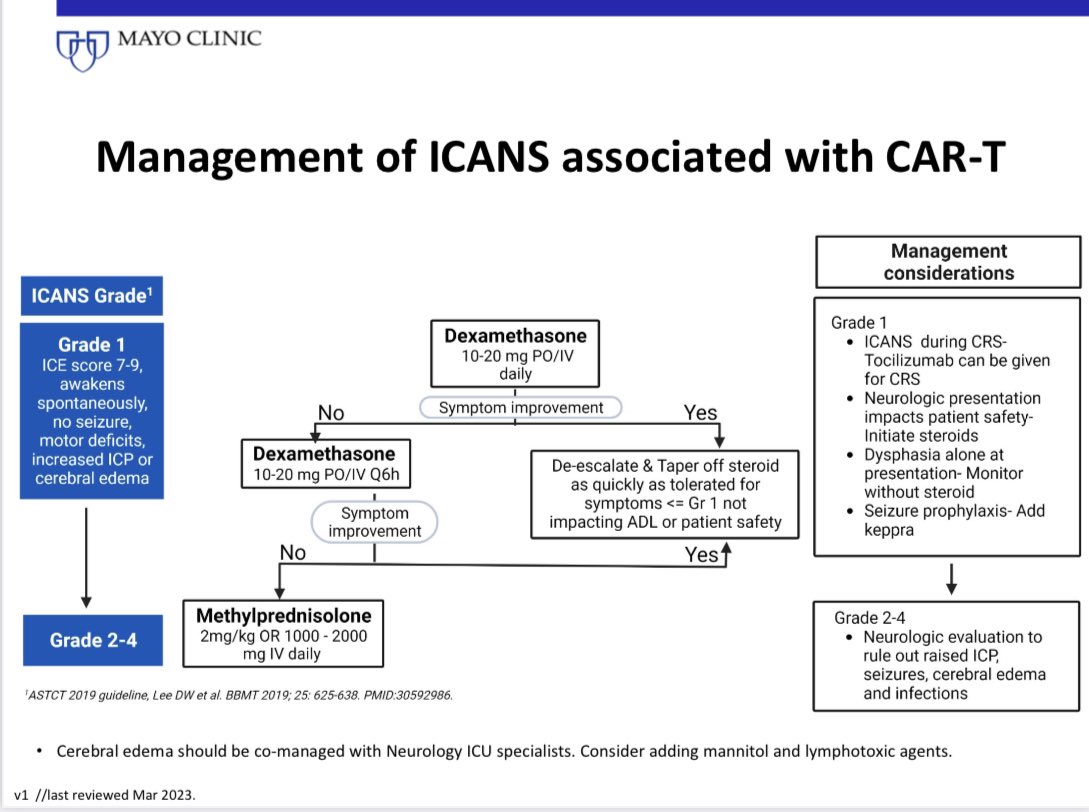
mSMART guidelines for management of CAR-T associated cytokine release syndrome, neurotoxicity, cytopenias has just been posted. #myeloma #MedTwitter
@YiLinMDPhD @myelomaMD @MorieGertz @MayoMyeloma
msmart.org
@YiLinMDPhD @myelomaMD @MorieGertz @MayoMyeloma
msmart.org
CAR-T associated CRS #ASCO23
CAR-T associated neurotoxicity #ASCO23

Are you ready for an #ASCO23 myeloma megathread? Here are 10 important abstracts to tune into to learn more (esp. with so little data in the abstract!). Let's go! #mmsm
Abstract 8000: Elo-KRd vs. KRd induction showed sig. improvement in MRD-neg rate (50% vs 35%) at end of induction. Long-term f/u + PFS data will be key. Might there be something about Elo and K synergy? Would this allow for using anti-CD38 mAb later? meetings.asco.org/abstracts-pres…
Abstract 8002: Teclistamab + talquetamab in RRMM.
➡️63 pts, 33% HR cyto, 78% triple-class refract., 43% extramed. dz.
⏲️14.4 mos f/u
🚨ORR 84% (73% in EMD)
🛟81% CRS (3% G3), 1 ICANS, 2 DLTs
Impressive ORR - what is durability? Better than sequential?
meetings.asco.org/abstracts-pres…
➡️63 pts, 33% HR cyto, 78% triple-class refract., 43% extramed. dz.
⏲️14.4 mos f/u
🚨ORR 84% (73% in EMD)
🛟81% CRS (3% G3), 1 ICANS, 2 DLTs
Impressive ORR - what is durability? Better than sequential?
meetings.asco.org/abstracts-pres…

Picture this:
A patient presents with an enlarging neck mass, and you find this 👇 on your evaluation.
What’s going on? 🤔
A #tweetorial 🧵 1/8
A patient presents with an enlarging neck mass, and you find this 👇 on your evaluation.
What’s going on? 🤔
A #tweetorial 🧵 1/8


To guide our thoughts, let’s start with two Hodgkin lymphoma (HL) facts-
1) Cancer cells can ⬆️ PD-L1, which interacts with T-cells’ PD-1 and ⬇️ immune activity
2) 🔑 Immune checkpoint inhibitors (ICIs) block the PD-1/PD-L1 interaction & have strong activity in HL 👇
🧵 2/8
1) Cancer cells can ⬆️ PD-L1, which interacts with T-cells’ PD-1 and ⬇️ immune activity
2) 🔑 Immune checkpoint inhibitors (ICIs) block the PD-1/PD-L1 interaction & have strong activity in HL 👇
🧵 2/8

Why do immune checkpoint inhibitors have such strong activity in HL? 🤔
🧵 3/8
🧵 3/8

In May 2019, Dr. @rschilsky & I co-chaired the #AAADV19 Workshop Plenary Session "Decentralized #ClinicalTrials: The Future is Now." An incredible group of panelists from academia, industry, govt, & patient #advocacy 👇discussed the rationale, challenges, & opportunities of DCTs.
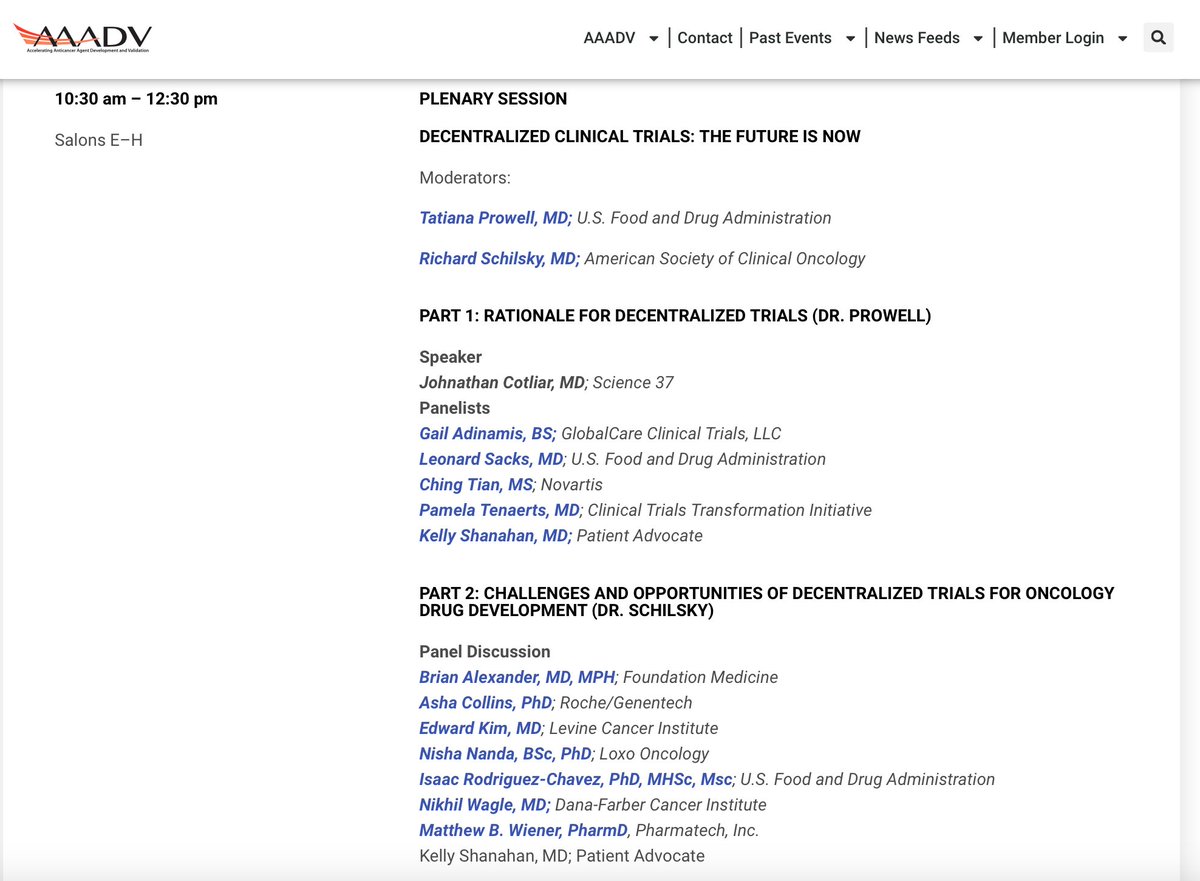
No one knew yet that the #COVID19 #pandemic was just around the corner. In Mar 2020, FDA released a guidance on conduct of #clinicaltrials during the pandemic: fda.gov/media/136238/d…, & colleagues wrote about the impact on #OncTwitter trials: ncbi.nlm.nih.gov/pmc/articles/P…. /2
FDA has now released a draft guidance on decentralized #clinicaltrials for drugs, biological products, & devices covering #telehealth, remote assessments, consent, shipping of IP, & more: fda.gov/media/167696/d…. #MedTwitter #regulatory #drugdevelopment


Hmmm. I am noticing that ex-US trials are not reporting race... Should this be a required element for @ASCO presentations?

Study design of MITO-23

MITO23 endpoints:
Primary: Overall Survival
Secondary: Progression Free Survival
Very interesting that OS was the primary endpoint I think...
Primary: Overall Survival
Secondary: Progression Free Survival
Very interesting that OS was the primary endpoint I think...
