Discover and read the best of Twitter Threads about #JanuAirway
Most recents (24)

Social Media for Anaesthetists.
Talk delivered at the beautiful Josef Chromy Winery in Launceston, Tasmania, Australia.
#ACE22TAS
Talk delivered at the beautiful Josef Chromy Winery in Launceston, Tasmania, Australia.
#ACE22TAS

Social media is enormous no matter how you look at it. Billions in ad revenue, millions of tweets every day, hours of our time on platforms. Pervasive in our personal and professional lives. Can't separate ourselves from it now.
(In the break one delegate proudly announced that they were in the minority - no social media at all.
I asked them if on WhatsApp .... yes but that's not social media they said .... 😬 .... we're on it, and we don't even know it sometimes ...)
I asked them if on WhatsApp .... yes but that's not social media they said .... 😬 .... we're on it, and we don't even know it sometimes ...)

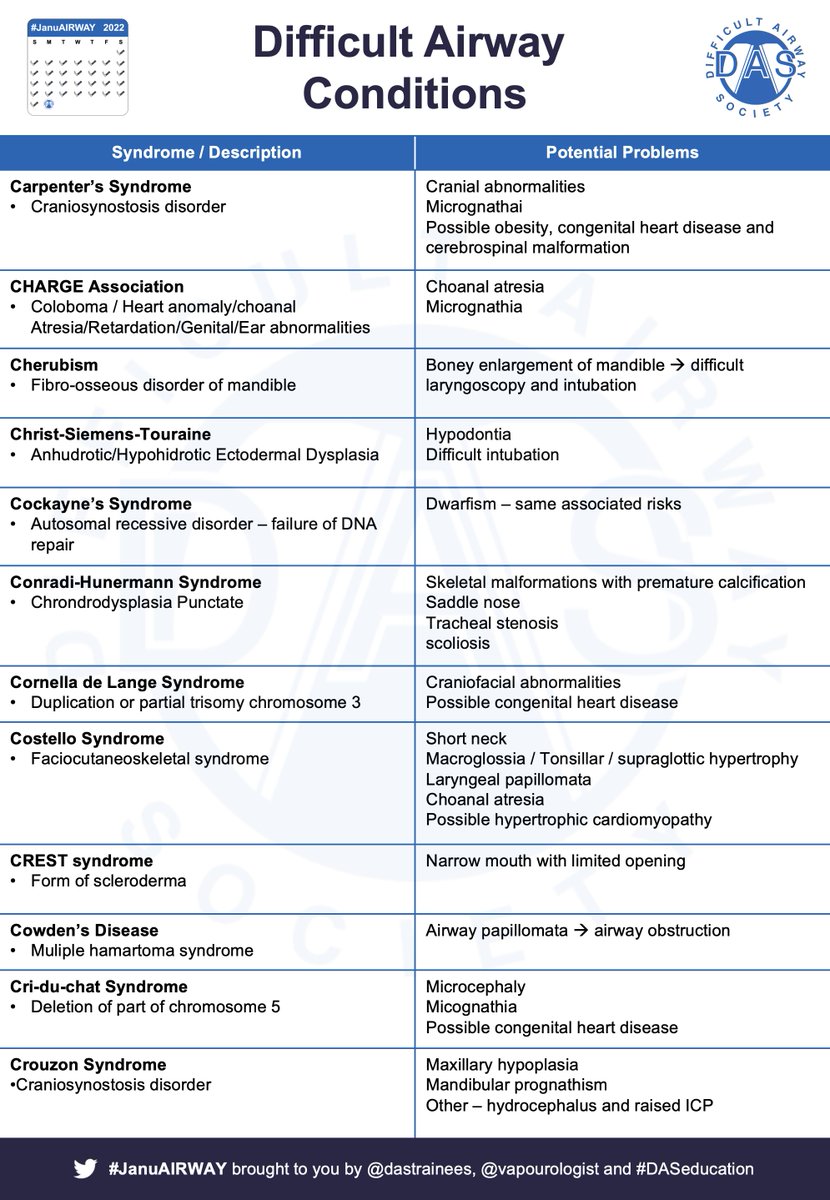
#JanuAIRWAY Day 31 (the last day!) – Difficult Airway Conditions. There are loads – what follows isn’t a definitive list – but it’s pretty long all the same! Let’s dive in…
#DifficultAirway #FOAMed
#JanuAIRWAY 1/7
#DifficultAirway #FOAMed
#JanuAIRWAY 1/7

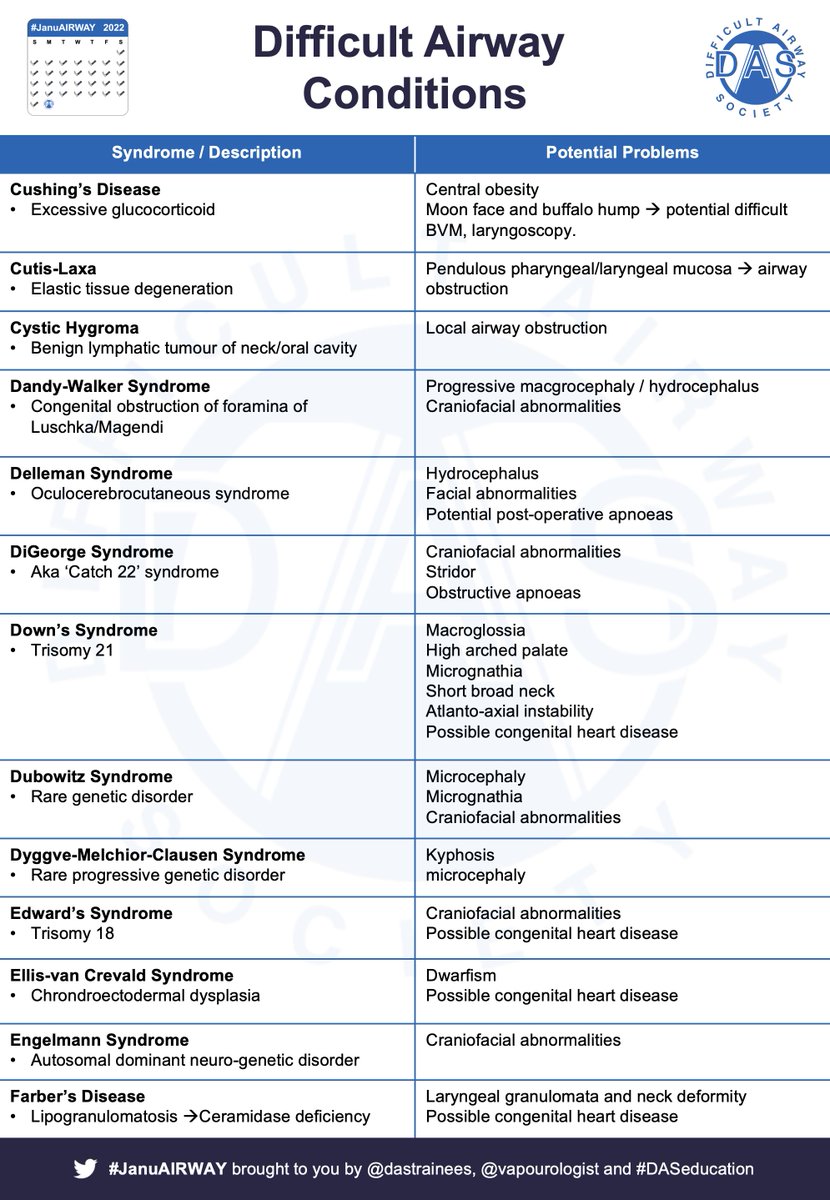

They keep coming! #JanuAIRWAY #FOAMed #DifficultAirways #Eponyms #Anaesthesia #Syndromes
#JanuAIRWAY 2/7
#JanuAIRWAY 2/7





#JanuAIRWAY Day 27 – The Neurosurgical Airway (thanks to @gasgal13 for her expert contribution to today’s content!). Head Vs Spine. Elective Vs Emergency. So many points of interest for airway managers. Here's a pair of #OnePagers to kick off!
#JanuAIRWAY 1/5
#JanuAIRWAY 1/5


Key principles:
- Prevent rises in ICP
- Avoid hypoxia & low BP
- Minimise C-spine movement where indicated
- Be aware of positioning
- Beware of potential difficult airway in neurosurgical pathology
- Beware of post-op issues e.g. haematoma post-ACDF
#JanuAIRWAY 2/5
- Prevent rises in ICP
- Avoid hypoxia & low BP
- Minimise C-spine movement where indicated
- Be aware of positioning
- Beware of potential difficult airway in neurosurgical pathology
- Beware of post-op issues e.g. haematoma post-ACDF
#JanuAIRWAY 2/5
We can, in general, divide acute / emergency patients into 2 groups:
1) Cooperative – awake techniques may be the best option in anticipated difficulty
2) Uncooperative – asleep laryngoscopy or asleep FOI (consider LMA conduit)
#FOAMed #JanuAIRWAY 3/5
1) Cooperative – awake techniques may be the best option in anticipated difficulty
2) Uncooperative – asleep laryngoscopy or asleep FOI (consider LMA conduit)
#FOAMed #JanuAIRWAY 3/5
#JanuAIRWAY Day 26 – The Traumatic Airway. Particularly stressful airways to manage = one part of a wider critically ill patient. Let’s kick off with a #OnePager
#FOAMed #JanuAIRWAY 1/5
#FOAMed #JanuAIRWAY 1/5

The principles of Rx are:
-Beware the isolated environment
-Plan for uncooperative patient
-Prevent aspiration
-Protect C-spine
-Plan for difficult airway
#FOAMed #JanuAIRWAY 2/5
-Beware the isolated environment
-Plan for uncooperative patient
-Prevent aspiration
-Protect C-spine
-Plan for difficult airway
#FOAMed #JanuAIRWAY 2/5
Define type of trauma early – blunt vs penetrating (neck divided into 3 zones), and assess for:
-Distorted anatomy
-Bleeding
-Subcut. Emphysema – injury to gas containing structure
-Other traumatic injury – e.g. head, thorax, abdomen, etc
#FOAMed #JanuAIRWAY 3/5
-Distorted anatomy
-Bleeding
-Subcut. Emphysema – injury to gas containing structure
-Other traumatic injury – e.g. head, thorax, abdomen, etc
#FOAMed #JanuAIRWAY 3/5

#JanuAIRWAY Day 25 – Obstetric Airways (thanks to @noolslucas for her expert contribution to todays content!). Let’s dive in…Here's a #OnePager and decision tools from a great review article
🔗doi.org/10.1111/anae.1…
#JanuAIRWAY 1/5
🔗doi.org/10.1111/anae.1…
#JanuAIRWAY 1/5




Failed intubation requires a different approach in Obs. The 2015 @dasairway /@OAAinfo guidelines are really helpful for this! Covering safe Obs GA, failed intubation and GA.
#JanuAIRWAY 2/5
#JanuAIRWAY 2/5




The DAS/OAA guidelines also cover decision making – when to bail out / when to proceed and aftercare – which mustn’t be overlooked!
#JanuAIRWAY 3/5
#JanuAIRWAY 3/5


#JanuAIRWAY Day 24 -Paediatric Airways. (ft. expert contributions from Alistair Baxter and @ENT_UK’s Adam Donne). Let’s dive in … Here's some #OnePagers covering anatomy, induction, airway manoeuvres and basic airway equipment.
#JanuAIRWAY 1/10
#JanuAIRWAY 1/10




Top tip from Alistair Baxter: Remember that a Macintosh blade is a hyperangulated blade in an infant and requires an intubation stylet shaped to match the curve of the blade
#JanuAIRWAY 2/10
#JanuAIRWAY 2/10
The difficult paediatric airway = #SCARY. Upper airway obstruction in children – broad range of presentations, three important diagnoses; Croup, Epiglottitis and Inhaled Foreign Body. Here’s some #OnePagers.
#JanuAIRWAY 3/10
#JanuAIRWAY 3/10


#JanuAIRWAY Day 23 (the final stretch!). Malacias and SVC Obstruction. Here's a pair of #OnePagers to get started..
#JanuAIRWAY 1/10
#JanuAIRWAY 1/10


What are malacias? = rare dynamic airway obstruction - (congenital / acquired) due to loss of cartilaginous support
Decreased intratracheal pressure + increased intrathoracic pressure lead to airway compression
Severity is proportional to expiratory force
#JanuAIRWAY 2/10
Decreased intratracheal pressure + increased intrathoracic pressure lead to airway compression
Severity is proportional to expiratory force
#JanuAIRWAY 2/10
Issues
Obstruction can occur even if aymptomatic
Maintain spont. Vent. if poss
Emergency management =+ve pressure (splint airways open) or bypass obstruction
Surgery depends on location / extent
Extubate deep (avoid coughing) or directly to CPAP
#JanuAIRWAY 3/10
Obstruction can occur even if aymptomatic
Maintain spont. Vent. if poss
Emergency management =+ve pressure (splint airways open) or bypass obstruction
Surgery depends on location / extent
Extubate deep (avoid coughing) or directly to CPAP
#JanuAIRWAY 3/10
#JanuAIRWAY Day 22. Airway Obstruction – Infraglottic (intrathoracic). Again, presents its own set of challenges. Let’s dive in … Here's a #OnePager (Ft. expert contribution Sadie Khwaja @ENT_UK )
#JanuAIRWAY 1/7
#JanuAIRWAY 1/7

Issues:
- Upper/Mid lesions usually low risk – ETT may pass beyond
- Low tracheal/Bronchial lesions = high risk, best managed in specialist centres
- CT scan = essential
- Sudden obstruction can occur at ANY time
- Potential compression of heart/vessels
#JanuAIRWAY 2/7
- Upper/Mid lesions usually low risk – ETT may pass beyond
- Low tracheal/Bronchial lesions = high risk, best managed in specialist centres
- CT scan = essential
- Sudden obstruction can occur at ANY time
- Potential compression of heart/vessels
#JanuAIRWAY 2/7
Severe Obstruction:
- Check position patient breaths best in
- Spont vent may help, IPPV may cause airway collapse
- Opinion re: IV vs inhalational = mixed
- Ketamine ?preserves chest wall tone
- Need back up plan
- Consider Heliox/bypass/ECMO before starting
#JanuAIRWAY 3/7
- Check position patient breaths best in
- Spont vent may help, IPPV may cause airway collapse
- Opinion re: IV vs inhalational = mixed
- Ketamine ?preserves chest wall tone
- Need back up plan
- Consider Heliox/bypass/ECMO before starting
#JanuAIRWAY 3/7
And just like that we’re 3 weeks into #JanuAIRWAY. Here’s your week 3 round up!
Day 15 – Tracheostomies
Day 16 – CICO Needle Techniques
Day 17 – CICO Scalpel Techniques
#JanuAIRWAY 1/4
Day 15 – Tracheostomies
Day 16 – CICO Needle Techniques
Day 17 – CICO Scalpel Techniques
#JanuAIRWAY 1/4

Day 18 – CICO Extra Equipment
Day 19 – The Obstructed Airway: Supraglottic
Day 20 – The Obstructed Airway: Periglottic
#JanuAIRWAY 2/4
Day 19 – The Obstructed Airway: Supraglottic
Day 20 – The Obstructed Airway: Periglottic
#JanuAIRWAY 2/4
Day 21 – The Obstructed Airway: Infraglottic Extrathoracic
Week 4 starts tomorrow continuing the theme of obstructed airways with Infraglottic Intrathoracic Obstruction. See you then!
#JanuAIRWAY 3/4
Week 4 starts tomorrow continuing the theme of obstructed airways with Infraglottic Intrathoracic Obstruction. See you then!
#JanuAIRWAY 3/4
#JanuAIRWAY Day 21. Airway Obstruction – Infraglottic (extrathoracic). Presents a unique set of challenges. Let’s dive in … Here's a #OnePager
#JanuAIRWAY 1/6
#JanuAIRWAY 1/6

Physiology
- Theory=fixed lesion unaffected by respiratory cycle / anaesthesia induction (most have dynamic element)
- Extrathoracic lesions usually better in expiration +ve pressure splints airway open
- Lets’ revisit flow-volume loops as they can be helpful
#JanuAIRWAY 2/6
- Theory=fixed lesion unaffected by respiratory cycle / anaesthesia induction (most have dynamic element)
- Extrathoracic lesions usually better in expiration +ve pressure splints airway open
- Lets’ revisit flow-volume loops as they can be helpful
#JanuAIRWAY 2/6

Issues:
- Laryngoscopy likely to be uneffected. However, major concern = inability to pass ETT atraumatically beyond the level of obstruction
- Nasendoscopy can be useful to view lesion
- AFOI/FOI may cause ‘cork in bottle’ effect depending on lesion size/location
#JanuAIRWAY 3/6
- Laryngoscopy likely to be uneffected. However, major concern = inability to pass ETT atraumatically beyond the level of obstruction
- Nasendoscopy can be useful to view lesion
- AFOI/FOI may cause ‘cork in bottle’ effect depending on lesion size/location
#JanuAIRWAY 3/6
#JanuAIRWAY Day 20. Airway Obstruction – Periglottic. Often the most challenging for the general anaesthetist. Let’s dive in … Here's a #OnePager
#JanuAIRWAY 1/6
#JanuAIRWAY 1/6

Issues:
- Must d/w with ENT colleagues
- Preop nasendoscopy by experienced nasendoscopist = essential
- AFOI may worsen obstruction – cork in bottle
- Inhalational induction may be difficult
Key Q's
- Static or dynamic obstruction?
- Will ETT pass?
#JanuAIRWAY 2/6
- Must d/w with ENT colleagues
- Preop nasendoscopy by experienced nasendoscopist = essential
- AFOI may worsen obstruction – cork in bottle
- Inhalational induction may be difficult
Key Q's
- Static or dynamic obstruction?
- Will ETT pass?
#JanuAIRWAY 2/6
Options:
- May be able to pass ETT – consider MLT or jet vent.
- Apnoeic (HFNO) or intermittent oxygenation technique depending on type of surgery (elective/emergent)
- Awake Tracheal Intubation
- Transtracheal catheter (+/- jet ventilation)
- Awake tracheostomy
#JanuAIRWAY 3/6
- May be able to pass ETT – consider MLT or jet vent.
- Apnoeic (HFNO) or intermittent oxygenation technique depending on type of surgery (elective/emergent)
- Awake Tracheal Intubation
- Transtracheal catheter (+/- jet ventilation)
- Awake tracheostomy
#JanuAIRWAY 3/6
#JanuAIRWAY Day 19. The Obstructed Airway – Think SPIMS
-Supra-
-Peri-
-Infra-glottic – extra/intrathoracic
-Malacias
-SVC Obstruction
Today we’re going to focus on Supraglottic Airway Obstruction. Here's a #OnePager to get started! #FOAMed
#JanuAIRWAY1/7
-Supra-
-Peri-
-Infra-glottic – extra/intrathoracic
-Malacias
-SVC Obstruction
Today we’re going to focus on Supraglottic Airway Obstruction. Here's a #OnePager to get started! #FOAMed
#JanuAIRWAY1/7

Possible issues:
-Risk of total obstruction with low tone
-Distorted anatomy
-NP/OP airway too short?
-+++jaw thrust may/may not relieve obstruction
-Difficult BVM/laryngoscopy
-+++ laryngoscopy may make manageable unmanageable (e.g.bleeding)
#FOAMed
#JanuAIRWAY 2/7
-Risk of total obstruction with low tone
-Distorted anatomy
-NP/OP airway too short?
-+++jaw thrust may/may not relieve obstruction
-Difficult BVM/laryngoscopy
-+++ laryngoscopy may make manageable unmanageable (e.g.bleeding)
#FOAMed
#JanuAIRWAY 2/7
Planning in airway obstruction = Key. NASENDOSCOPY can save lives here! ASSESSMENT informs STRATEGY. Let’s revisit some #OnePagers on key questions and airway planning. Remember the decision-making process is multifactorial (maintain situational awareness).
#JanuAIRWAY 3/7
#JanuAIRWAY 3/7



#JanuAIRWAY Day 18. Extra CICO Equipment. At least 2 pieces of equipment deserve extra attention – Rapid-O2 & the Melker airway (key components of the cannula technique one for initial oxygenation & one for securing the airway)! Here’s a pair of #OnePagers to get started.. 1/5


A bonus #OnePager on the QuickTrach airway – used for wide bore cricothyroidotomy, it may still lurk in a few departments throughout the land! Here’s a video as well #FOAMed
#JanuAIRWAY 2/5
#JanuAIRWAY 2/5

Double bonus #OnePager – on the Ventrain Device – a newer, but interesting, device! Can be used both electively & as part of CICO. Here’s a recent paper that highlights its potential read.qxmd.com/read/33432628/… #FOAMed
#JanuAIRWAY 3/5
#JanuAIRWAY 3/5

#JanuAIRWAY Day 17. CICO - Scalpel Techniques. Absolutely ESSENTIAL knowledge for anyone involved in airway management! Here’s a #OnePager with the @dasairway algorithm. Let’s dive in… #FOAMed
#JanuAIRWAY 1/6
#JanuAIRWAY 1/6

DAS advocates scalpel-bougie-tube technique for palpable anatomy and scalpel-finger-bougie-tube technique for impalpable anatomy. Here are some #OnePagers #FOAMed
#JanuAIRWAY 2/6
#JanuAIRWAY 2/6


Perhaps the most difficult part of the process is making the mental leap to pick up the scalpel. That's why mental models and thinking tools like the @VortexApproach are so useful. Check out @NicholasChrimes & Peter Fritz's work
🔗vortexapproach.org
#JanuAIRWAY 3/6
🔗vortexapproach.org
#JanuAIRWAY 3/6
#JanuAIRWAY Day 16 (we’re over ½ way!) Cannot Intubate Cannot Oxygenate (CICO) Scenario - Needle Techniques. Potentially controversial (DAS primarily advocates scalpel techniques), but worth knowing about - particularly for paeds! Here’s some #OnePagers to start..
#JanuAIRWAY 1/7
#JanuAIRWAY 1/7


CICO Key = decide on your plan before you're in the situation. @dasairway promotes scalpel techniques (final common pathway of CICO) MUST be taught. For more on the Needle technique check of Dr Andy Heard’s work at the Perth ‘wet’ lab. 🔗bjanaesthesia.org.uk/article/S0007-…
#JanuAIRWAY 2/7
#JanuAIRWAY 2/7
Integrating the needle technique into CICO algorithms could look something like this #OnePager. There are 2 scenarios for each technique (needle & scalpel):
-palpable and
-impalpable anatomy
another reason to decide early –> lower cognitive load. #FOAMed
#JanuAIRWAY 3/7
-palpable and
-impalpable anatomy
another reason to decide early –> lower cognitive load. #FOAMed
#JanuAIRWAY 3/7

#JanuAIRWAY Day 15. Tracheostomies – more than just an ETT through the neck. Here’s a #OnePager covering some of the different tube types. Let’s dive in…
#JanuAIRWAY 1/9
#JanuAIRWAY 1/9

Tracheostomies have potentially been performed since ancient Egypt. The first non-emergency trache was thought to be performed by Asclepiades. He was also a proponent of music therapy (might be of interest to Veena).
#JanuAIRWAY 2/9
#JanuAIRWAY 2/9

There are 4 basic indications for tracheostomy:
1. Provide patent airway
2. Protect the airway
3. Clear secretions
4. Aid weaning from ventilator – the timing of which was investigated in the Tracman study in 2013 (jama.jamanetwork.com/article.aspx?a…)
#JanuAIRWAY 3/9
1. Provide patent airway
2. Protect the airway
3. Clear secretions
4. Aid weaning from ventilator – the timing of which was investigated in the Tracman study in 2013 (jama.jamanetwork.com/article.aspx?a…)
#JanuAIRWAY 3/9
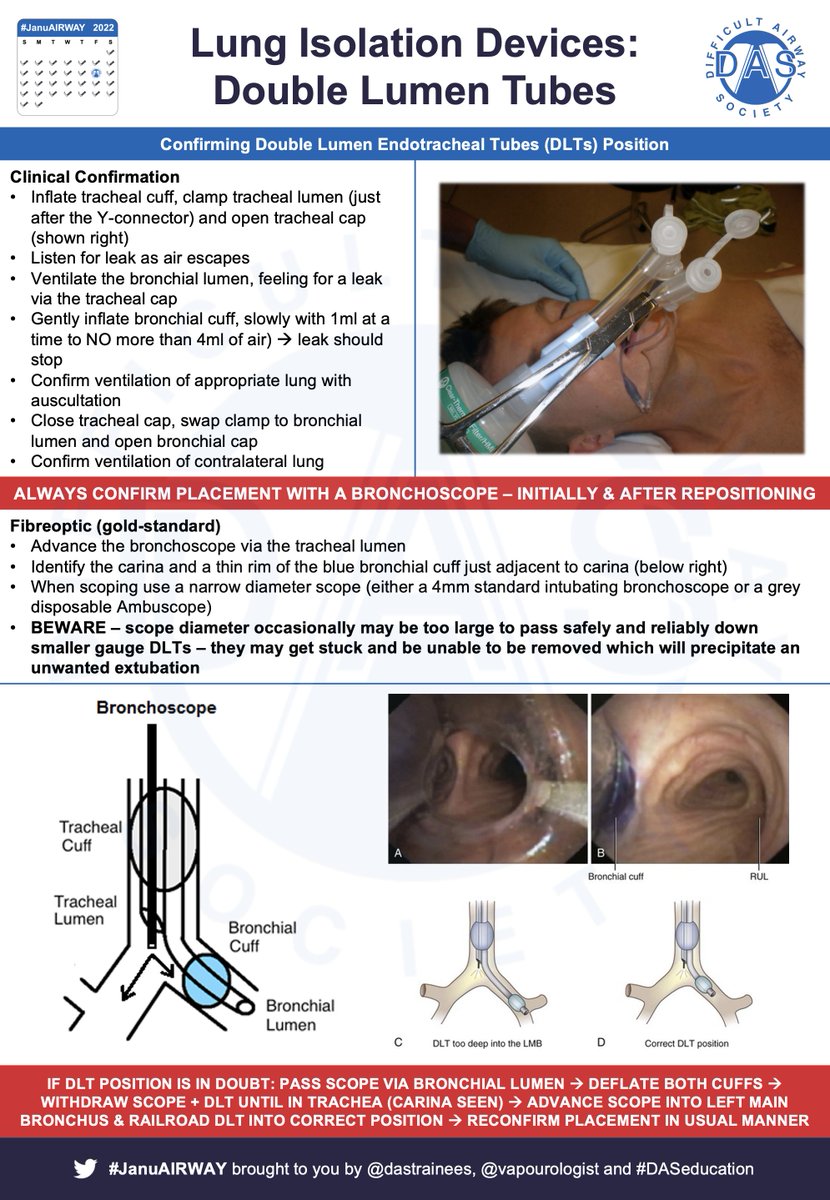
#JanuAIRWAY Day 14. One Lung Ventilation – one of @vapourologist’s favourite procedures in anaesthesia – physiology in action! Here’s a #OnePager. Let’s dive in…
#JanuAIRWAY 1/9
#JanuAIRWAY 1/9

Several indications for OLV, commonest are thoracic surgery & some oesophagectomies. Essentially three ways to achieve OLV - use of:
- Double lumen tube
- Bronchial Blocker
- Elective endobronchial intubation
Here are some #OnePagers covering the basics
#JanuAIRWAY 2/9
- Double lumen tube
- Bronchial Blocker
- Elective endobronchial intubation
Here are some #OnePagers covering the basics
#JanuAIRWAY 2/9



The key physiological change is the creation of a large shunt – deoxygenated blood (which would normally be oxygenated), returns to the left heart resulting in hypoxaemia.
#JanuAIRWAY 3/9
#JanuAIRWAY 3/9

#JanuAIRWAY Day 13. Jet Ventilation – this is a bit more niche in anaesthesia / airway management, but fascinating. Here’s a #OnePager covering the basics. Let’s dive in…
#JanuAIRWAY 1/8
#JanuAIRWAY 1/8

2 modes of jet ventilation – low frequency (<60 jets/min) & high frequency (>60). Frequency determines device. 2 commonly used devices – Manujet (modified hand operated Sanders injector) or Monsoon (specialised jet ventilator). Here’s a some #OnePagers
#JanuAIRWAY 2/8
#JanuAIRWAY 2/8



Several different potential mechanisms to apnoic oxygenation during HFJV, including:
-Bulk flow
-Laminar flow
-Taylor dispersion
-Pendelluft
-Molecular diffusion
-Cardiogenic mixing
derangedphysiology.com has a great article & this diagram #FOAMed
#JanuAIRWAY 3/8
-Bulk flow
-Laminar flow
-Taylor dispersion
-Pendelluft
-Molecular diffusion
-Cardiogenic mixing
derangedphysiology.com has a great article & this diagram #FOAMed
#JanuAIRWAY 3/8

#JanuAIRWAY Day 12. Awake Techniques (ft. expert contributions from @dr_imranahmad). This is a key skill for an airway manager. Here’s a #OnePager covering the basics of Awake Tracheal Intubation (ATI) and nasendoscopy. Let’s dive in…
#JanuAIRWAY 1/11
#JanuAIRWAY 1/11

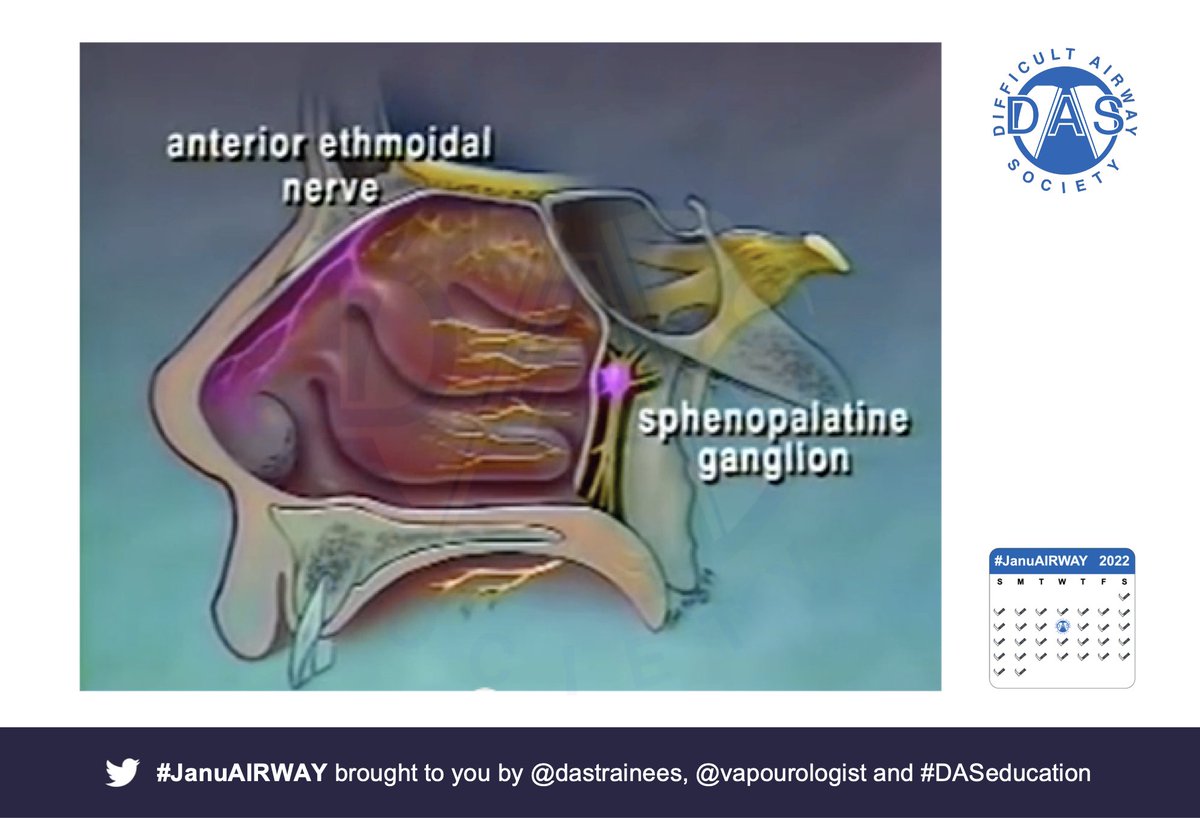
Key = topicalization (if right, may not need sedation). Top tips:
- Know nerve supply CN V, IX & X.
- Block Ant.ethmoidal AND Sphenopalatine ganglion supply to the nasal septum
#JanuAIRWAY 2/11
- Know nerve supply CN V, IX & X.
- Block Ant.ethmoidal AND Sphenopalatine ganglion supply to the nasal septum
#JanuAIRWAY 2/11

Often you don’t need high dose LA if in right spot – this video is @Vapourologist after only gargling instilagel.
#JanuAIRWAY 3/11
#JanuAIRWAY 3/11
#JanuAIRWAY Day 11. The Aintree Intubation Catheter – an amazingly useful piece of equipment – every airway practitioner should be familiar with. Here’s a #OnePager. Let’s dive in…
#JanuAIRWAY 1/5
#JanuAIRWAY 1/5

Main function is as a stop-gap to maintain tracheal access & facilitate tracheal intubation through a supraglottic airway device (SAD) using a fibreoptic scope. They are Long, hollow, semi-rigid, powder blue, polyurethane catheters
#JanuAIRWAY 2/5
#JanuAIRWAY 2/5


To highlight: NEVER insert beyond 26cm. NEVER insufflate with an oxygen flow >2l/min … or just NEVER use for insufflation!
#JanuAIRWAY 3/5
#JanuAIRWAY 3/5
#JanuAIRWAY Day 10. The Cook Airway Exchange Catheter – it’s a useful piece of equipment, but one not everyone will be familiar with. Here’s a #OnePager. Let’s dive in…
#JanuAIRWAY 1/6
#JanuAIRWAY 1/6

Main function is as a stop-gap to maintain tracheal access & facilitate ETT exchange. They are long, hollow, radiopaque, soft-tipped tubes – types for use with single / double lumen tubes.
#JanuAIRWAY 2/6
#JanuAIRWAY 2/6

All users MUST be trained & knowledgeable of how to use such devices together with their limitations and dangers. The Gordon Ewing case makes for tragic reading – but highlights this point. Essential reading for airway practitioners.
🔗scotcourts.gov.uk/search-judgmen…
#JanuAIRWAY 3/6
🔗scotcourts.gov.uk/search-judgmen…
#JanuAIRWAY 3/6
#JanuAIRWAY Day 9. High Flow Nasal Oxygen (HFNO). This has been a game-changer in recent years. Thank you A.Patel and S Nouraei for their amazing landmark paper on THRIVE! 🔗pubmed.ncbi.nlm.nih.gov/25388828/
Let’s dive in…
#JanuAIRWAY 1/6
Let’s dive in…
#JanuAIRWAY 1/6

Oxygen consumption continues during apnoea, gradual loss of alveolar volume/reduction in pressure. If upper airway remains patent, gas can be drawn into lower airways and oxygenation can continue and delay desaturation.
#JanuAIRWAY 2/6
#JanuAIRWAY 2/6


HFNO:
1. Reduces heat and moisture loss from the airway
2. Decreases anatomical deadspace
3. Provides PEEP
4. Improves Oxygenation
See this @BJAJournals article which summarises the physiological basis and clinical contraindications👇
🔗academic.oup.com/bjaed/article/…
#JanuAIRWAY 3/6
1. Reduces heat and moisture loss from the airway
2. Decreases anatomical deadspace
3. Provides PEEP
4. Improves Oxygenation
See this @BJAJournals article which summarises the physiological basis and clinical contraindications👇
🔗academic.oup.com/bjaed/article/…
#JanuAIRWAY 3/6
#JanuAIRWAY Day 8. Capnography. This is one of essential pieces of monitoring equipment needed during airway management. But its presence isn’t enough, correct interpretation is vital. Let’s start with a #OnePager looking at the different waveforms.
#JanuAIRWAY 1/10
#JanuAIRWAY 1/10

Oesophageal intubation still occurs & EtCO2 = key tool to help prevent avoidable deaths such as Glenda Logsdail’s. Key message = flat or no trace indicates oesophageal intubation until proven otherwise #NoTraceWrongPlace
#JanuAIRWAY 2/10
#JanuAIRWAY 2/10

This thread by @doctimcook is fantastic and we recommend everyone read it! #NoTraceWrongPlace
🔗
#JanuAIRWAY 3/10
🔗
#JanuAIRWAY 3/10
#JanuAIRWAY's off to a great start. Here’s a summary of Week One.
Day 1 – Oxygenation -
Day 2 – Assessment -
Day 3 – The Difficult Airway -
Day 4 – Investigations/Ultrasound -
1/2
Day 1 – Oxygenation -
Day 2 – Assessment -
Day 3 – The Difficult Airway -
Day 4 – Investigations/Ultrasound -
1/2

Day 5 – Planning -
Day 6 – Equipment -
Day 7 – Laryngoscopy -
Week 2 starts tomorrow with Capnography. See you then!
2/3
Day 6 – Equipment -
Day 7 – Laryngoscopy -
Week 2 starts tomorrow with Capnography. See you then!
2/3
*Disclaimer:Inclusion of content (equipment/ techniques/scoring systems/etc.) in #JanuAIRWAY does not constitute DAS endorsement.
3/3
3/3
